Derks Kris, Steenhuijsen Jacco L G, van den Berg Hetty A, Houterman Saskia, Cnossen Jeltsje, van Haaren Paul, De Jaeger Katrien
Department of Radiotherapy.
Department of Education and Research, Catharina Hospital, Eindhoven, The Netherlands.
J Contemp Brachytherapy. 2018 Feb;10(1):17-25. doi: 10.5114/jcb.2018.73955. Epub 2018 Feb 22.
The purpose of this study was to analyze the effect of 2D conventional brachytherapy (CBT) compared to 3D MRI-guided brachytherapy (IGBT) with and without the use of interstitial needles on local control, overall survival, and toxicity in patients treated for cervical cancer with radiation or chemoradiation.
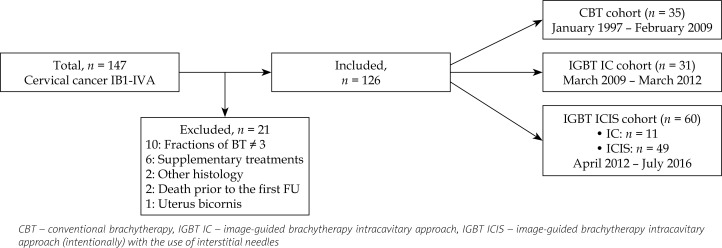
A retrospective analysis was performed of biopsy-proven FIGO IB-IVA cervical cancer patients, treated with primary radiation or chemoradiation, followed by brachytherapy (BT) between January 1997 and July 2016. Endpoints were local control, overall survival, and toxicity.
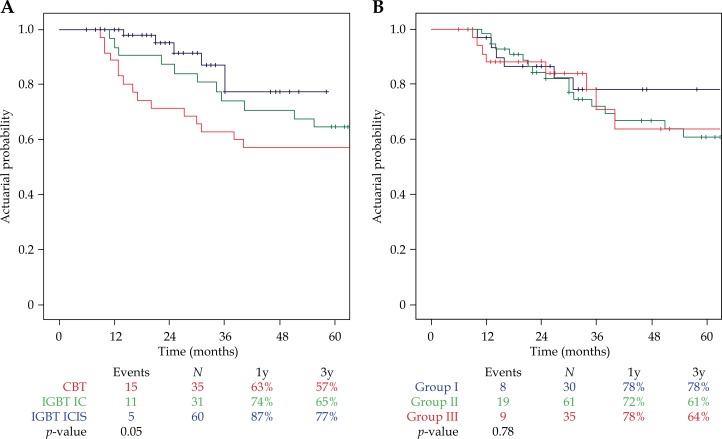
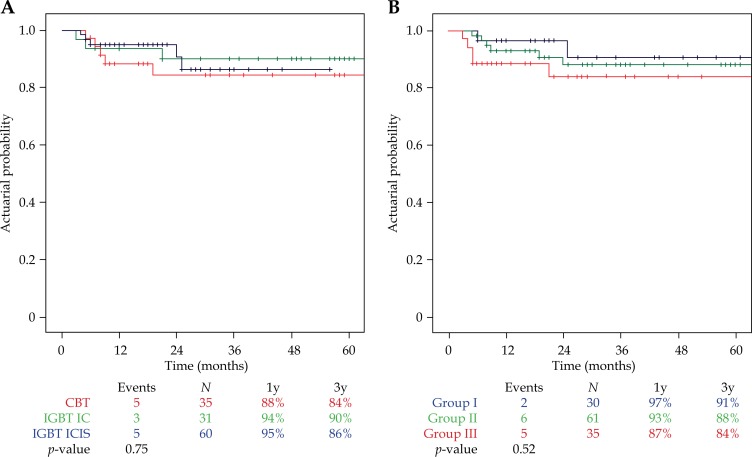
Of 126 patients included, 35 have been treated with CBT, 31 with IGBT without needles (IC), and 60 with IGBT with needles (ICIS). External beam radiotherapy (EBRT) had mostly been delivered concurrently with chemotherapy (weekly cisplatin). Overall local control was 93% after 1 year, and 88% after 3 years. Overall 3-year survival was 75%, and 5-year survival was 66%. The 3D technique (IGBT cohorts) showed a trend for an improved local control and overall survival ( = 0.05) compared to the 2D technique (CBT cohort). A decrease in toxicity was observed from 17% (2D cohort) to 12% (3D cohort). The use of interstitial needles was associated with a higher high-risk clinical target volume (HR-CTV) dose (11.3 Gy vs. 9.9 Gy) and a lower D bladder dose (10.9 Gy vs. 14.7 Gy, both < 0.01).
In cervical cancer treatment, the use of a 3D brachytherapy technique (MRI-guided with or without interstitial needles) showed a trend towards an increased local control and improved overall survival with reduced toxicity, compared to the conventional 2D brachytherapy technique. The use of interstitial needles allowed dose sculpting, resulting in delivery of higher doses to the HR-CTV, while reducing radiation doses to organs at risk, such as the bladder.
本研究旨在分析二维传统近距离放射治疗(CBT)与三维磁共振成像引导近距离放射治疗(IGBT)在使用或不使用组织间插植针的情况下,对接受放疗或放化疗的宫颈癌患者局部控制、总生存期和毒性的影响。
对1997年1月至2016年7月间经活检证实为国际妇产科联盟(FIGO)IB-IVA期宫颈癌且接受了初始放疗或放化疗,随后接受近距离放射治疗(BT)的患者进行回顾性分析。观察终点为局部控制、总生存期和毒性。
纳入的126例患者中,35例接受了CBT,31例接受了无针IGBT(IC),60例接受了有针IGBT(ICIS)。外照射放疗(EBRT)大多与化疗(每周顺铂)同步进行。1年后总体局部控制率为93%,3年后为88%。3年总生存率为75%,5年生存率为66%。与二维技术(CBT队列)相比,三维技术(IGBT队列)在局部控制和总生存期方面显示出改善趋势(P = 0.05)。毒性从17%(二维队列)降至12%(三维队列)。组织间插植针的使用与更高的高危临床靶区体积(HR-CTV)剂量(11.3 Gy对9.9 Gy)和更低的膀胱D剂量(10.9 Gy对14.7 Gy,均P < 0.01)相关。
在宫颈癌治疗中,与传统二维近距离放射治疗技术相比,使用三维近距离放射治疗技术(磁共振成像引导,有或无组织间插植针)显示出局部控制增加、总生存期改善且毒性降低的趋势。组织间插植针的使用允许剂量塑形,从而在向HR-CTV输送更高剂量的同时,降低对膀胱等危及器官的辐射剂量。