Kusada Takeaki, Toita Takafumi, Ariga Takuro, Maemoto Hitoshi, Hashimoto Seiji, Shiina Hideki, Kakinohana Yasumasa, Heianna Joichi, Nagai Yutaka, Kudaka Wataru, Aoki Yoichi, Murayama Sadayuki
Department of Radiology, Graduate School of Medical Science, University of the Ryukyus, 207 Uehara, Nishihara, Okinawa 903-0215, Japan.
Radiation Therapy Center, Okinawa Chubu Hospital, 281 Miyazato, Uruma, Okinawa 904-2293, Japan.
J Radiat Res. 2018 Jan 1;59(1):67-76. doi: 10.1093/jrr/rrx065.
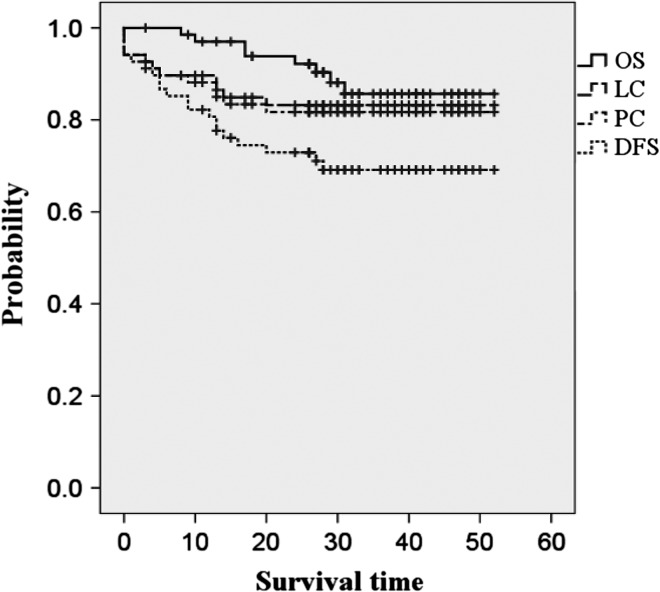
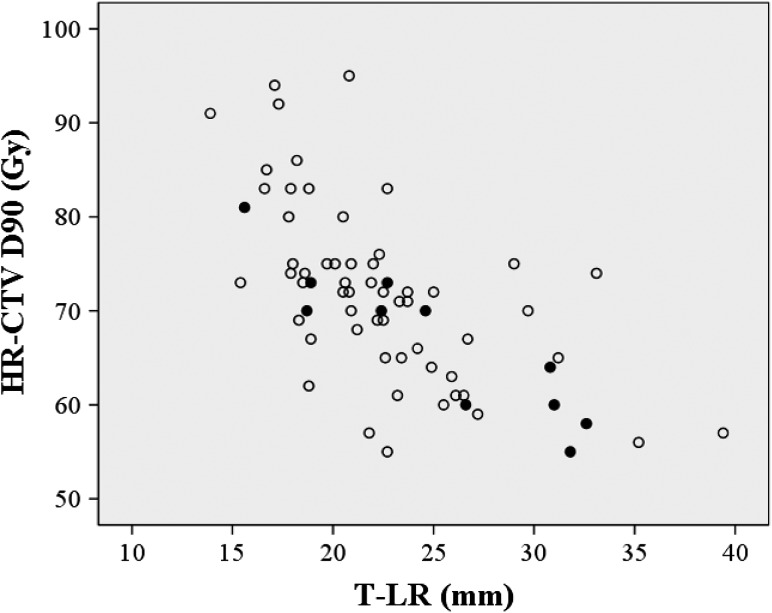
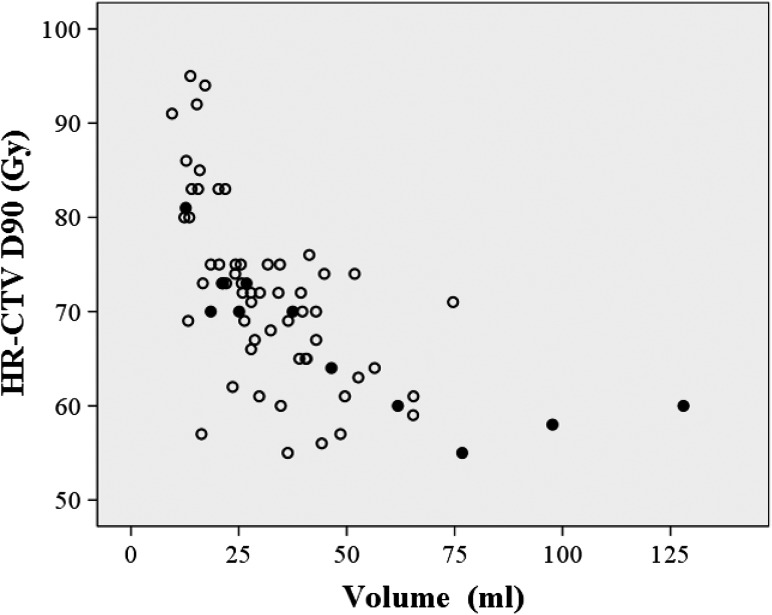
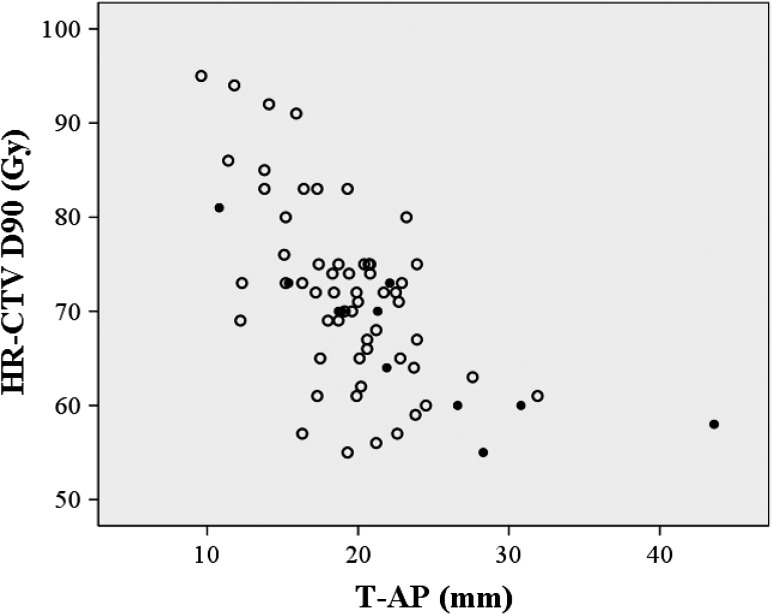
This study evaluated the oncologic outcomes and complications of cervical cancer patients in terms of CT-based image-guided brachytherapy (IGBT) parameters. Of 68 cervical cancer patients treated with definitive radiotherapy/concurrent chemoradiotherapy, most received whole-pelvis external beam RT (EBRT) of 40 Gy in 20 fractions, pelvic EBRT with central shield of 10 Gy in 5 fractions, and CT-based IGBT of 18 Gy in 3 fractions prescribed to point A. Cumulative EBRT and IGBT doses were calculated as the total equivalent dose in 2 Gy fractions (EQD2). The median follow-up was 31 (3-52) months. The 2-year overall survival, local control, pelvic control, and disease-free survival rates of the 68 patients were 92%, 83%, 82% and 73%, respectively. The HR-CTV D90, length from the tandem axis to left/right margin of the HR-CTV (T-LR), and HR-CTV volume were significant IGBT parameters for predicting local/pelvic control. Patients who received an HR-CTV D90 of >60 Gy, compared with ≤60 Gy, had significantly better local/pelvic control. Furthermore, 70 Gy was a marginally significant HR-CTV D90 cut-off affecting local control. T-LR was an independent IGBT parameter predicting local/pelvic control on multivariate analysis. Three patients developed Grade 3 or higher treatment-related complications. The D2cm3 of organs at risk were not significant predictors of complications. Future challenges for further improving outcomes include additional interstitial needles for irregularly shaped HR-CTVs, and moderate dose escalation, especially for patients with poor tumor responses.
本研究根据基于CT的图像引导近距离放射治疗(IGBT)参数评估了宫颈癌患者的肿瘤学结局和并发症。在68例接受根治性放疗/同步放化疗的宫颈癌患者中,大多数患者接受了20次分割、总量40 Gy的全盆腔外照射放疗(EBRT),5次分割、总量10 Gy的盆腔中央遮挡EBRT,以及针对A点的3次分割、总量18 Gy的基于CT的IGBT。累积EBRT和IGBT剂量计算为2 Gy分割的总等效剂量(EQD2)。中位随访时间为31(3 - 52)个月。这68例患者的2年总生存率、局部控制率、盆腔控制率和无病生存率分别为92%、83%、82%和73%。HR-CTV D90、从串联轴到HR-CTV左/右边缘的长度(T-LR)以及HR-CTV体积是预测局部/盆腔控制的重要IGBT参数。与HR-CTV D90≤60 Gy的患者相比,接受HR-CTV D90>60 Gy的患者具有显著更好的局部/盆腔控制。此外,70 Gy是影响局部控制的边缘显著的HR-CTV D90临界值。在多变量分析中,T-LR是预测局部/盆腔控制的独立IGBT参数。3例患者发生3级或更高等级的治疗相关并发症。危及器官的D2cm3不是并发症的显著预测因素。进一步改善结局的未来挑战包括为形状不规则的HR-CTV增加间质针,以及适度增加剂量,特别是对于肿瘤反应较差的患者。