Radwan Hanan I
Faculty of Medicine, Zagazig University, Cardiovascular Department, Egypt.
Egypt Heart J. 2017 Mar;69(1):1-11. doi: 10.1016/j.ehj.2016.05.004. Epub 2016 Jun 16.
Left atrium (LA) dilatation has been associated with adverse cardiovascular outcomes in patients with sinus rhythm and atrial fibrillation (AF).
We aimed to evaluate the accuracy of left atrial (LA) size to predict transesophageal echocardiographic (TEE) markers of increased thromboembolic risk left atrial appendage (LAA) thrombus, low LAA velocities and dense spontaneous echocardiographic contrast (SEC), and also to assess the best method to evaluate LA size.
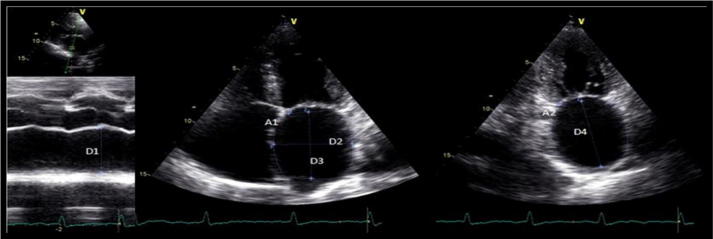
Cross-sectional study included 64 patients with nonvalvular AF undergoing transthoracic and transesophageal echocardiographic (TTE and TEE) evaluation. LA size was measured on TTE by several methods including the following: anteroposterior diameter (AP), LA area in four and two apical chamber views and volumes by ellipsoid, single plane (1P) and biplane area-length (2P) formulas. All these measures were indexed to the body surface area (BSA). Thromboembolic markers including LAA thrombus, low LAA velocities, dense SEC and LA abnormality (LA ABN) which means the presence of one or more of the previous three parameters were evaluated by TEE.
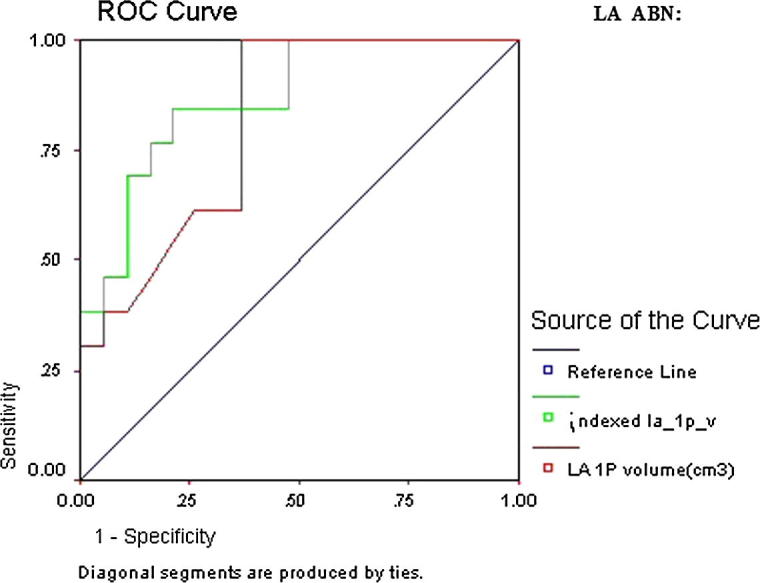
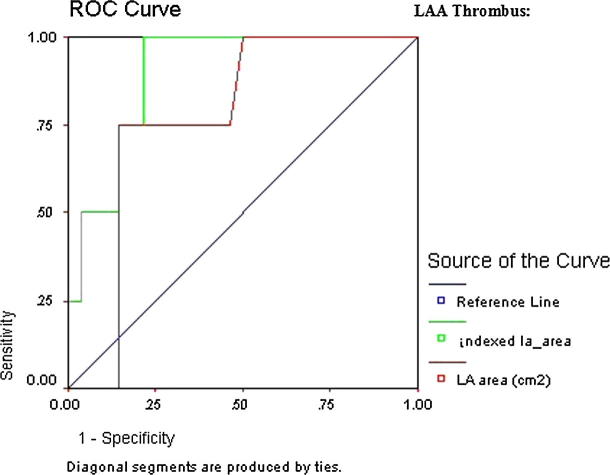
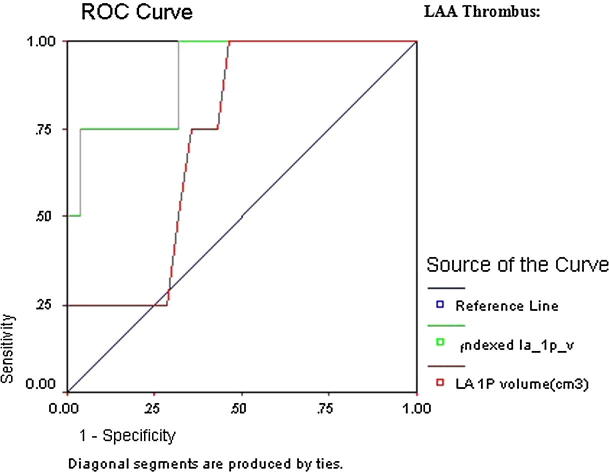
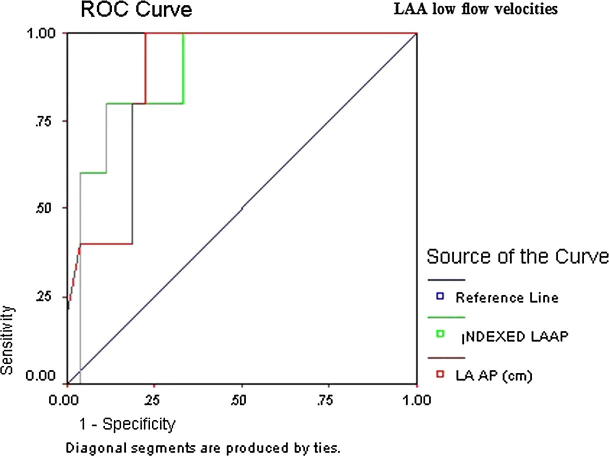
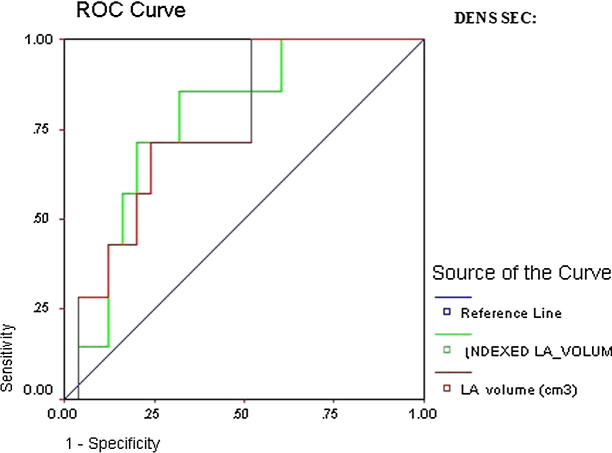
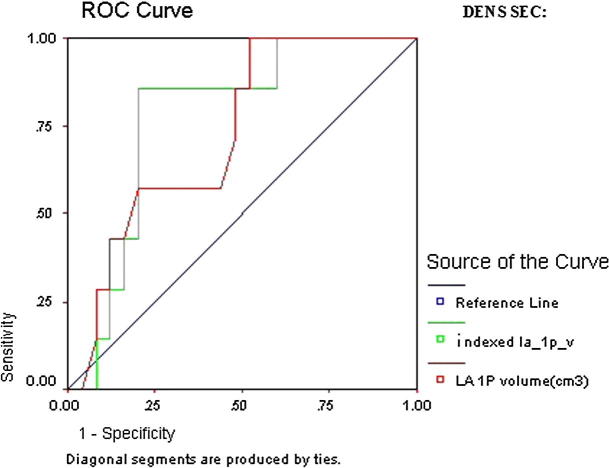
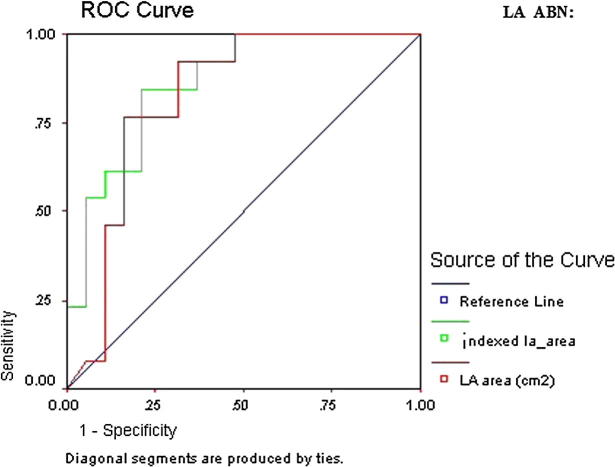
There was statistically significant increase in indexed and non-indexed LA parameters in patients with LA ABN compared to patients without LA ABN. According to ROC curve, the study found that all indexed LA parameters were predictive for LAA thrombus with the highest AUC was indexed LA 1P area length volume (AUC 0.91, CI 95% 0.81-1.01, < 0.000), for LAA low flow velocity were indexed and non-indexed LA AP diameters with the highest AUC was indexed LA AP diameter (AUC 0.89, CI 95% 0.80-0.98, < 0.000), for LA dense SEC were indexed LA ellipsoid volume (AUC 0.78, CI 95% 0.66-0.96, = 0.002) and indexed LA 1P area length volume (AUC 0.78, CI 95% 0.66-0.90, = 0.002) and for LA ABN were all LA parameters with the highest AUC was indexed LA 1P area length volume (AUC 0.87, CI 95% 0.79-0.96, < 0.000). On multivariate logistic regression analysis of TEE parameters, the study found that the most predictive LA measurement for LAA thrombus was indexed LA AP diameter with cutoff 3 cm/m (OR 7.5, 95% CI 1.24-45.2, = 0.02), for LAA low flow velocity was LA AP diameter with cutoff 6 cm (OR 17.6, 95% CI 3.23-95.84, = 0.001), for LA dense SEC was indexed LA ellipsoid volume with cutoff 42 cm/m (OR 6.5, 95% CI 1.32-32.07, = 0.02), and for LA ABN was indexed LA ellipsoid volume with cutoff 42 cm/m (OR 10.45, 95% CI 2.18-51.9, = 0.008).
LA enlargement is suitable to predict thromboembolic markers in patients with non-valvular AF. The indexed and non-indexed LA AP diameter and indexed LA ellipsoid volume were the most accurate parameters for predicting thromboembolic markers.
左心房(LA)扩张与窦性心律和心房颤动(AF)患者的不良心血管结局相关。
我们旨在评估左心房(LA)大小预测经食管超声心动图(TEE)血栓栓塞风险增加标志物的准确性,这些标志物包括左心耳(LAA)血栓、LAA低流速和密集的自发超声造影(SEC),并评估评估LA大小的最佳方法。
横断面研究纳入了64例接受经胸和经食管超声心动图(TTE和TEE)评估的非瓣膜性AF患者。通过多种方法在TTE上测量LA大小,包括以下方法:前后径(AP)、四腔心和两腔心尖视图中的LA面积以及通过椭圆体、单平面(1P)和双平面面积-长度(2P)公式计算的容积。所有这些测量值均根据体表面积(BSA)进行指数化。通过TEE评估血栓栓塞标志物,包括LAA血栓、LAA低流速、密集的SEC和LA异常(LA ABN),LA ABN是指存在上述前三个参数中的一个或多个。
与无LA ABN的患者相比,有LA ABN的患者的指数化和非指数化LA参数有统计学显著增加。根据ROC曲线,研究发现所有指数化的LA参数对LAA血栓都有预测性,AUC最高的是指数化LA 1P面积长度容积(AUC 0.91,95%CI 0.81-1.01,<0.000);对于LAA低流速,指数化和非指数化的LA AP直径有预测性,AUC最高的是指数化LA AP直径(AUC 0.89,95%CI 0.80-0.98,<0.000);对于LA密集SEC,指数化LA椭圆体容积(AUC 0.78,95%CI 0.66-0.96,=0.002)和指数化LA 1P面积长度容积(AUC 0.78,95%CI 0.66-0.90,=0.002)有预测性;对于LA ABN,所有LA参数都有预测性,AUC最高的是指数化LA 1P面积长度容积(AUC 0.87,95%CI 0.79-0.96,<0.000)。在对TEE参数进行多因素逻辑回归分析时,研究发现预测LAA血栓最具预测性的LA测量值是指数化LA AP直径,截断值为3 cm/m²(OR 7.5,95%CI 1.24-45.2,=0.02);对于LAA低流速,是LA AP直径,截断值为6 cm(OR 17.6,95%CI 3.23-95.84,=0.001);对于LA密集SEC,是指数化LA椭圆体容积,截断值为42 cm/m²(OR 6.5,95%CI 1.32-32.07,=0.02);对于LA ABN,是指数化LA椭圆体容积,截断值为42 cm/m²(OR 10.45,95%CI 2.18-51.9,=0.008)。
LA扩大适用于预测非瓣膜性AF患者的血栓栓塞标志物。指数化和非指数化的LA AP直径以及指数化LA椭圆体容积是预测血栓栓塞标志物最准确的参数。