Department of Obstetrics and Gynecology, University of Utah Health, Salt Lake City, UT; Women and Newborns Clinical Program, Intermountain Healthcare, Salt Lake City, UT.
Population Sciences, Huntsman Cancer Institute, University of Utah Health, Salt Lake City, UT.
Am J Obstet Gynecol. 2018 Jul;219(1):107.e1-107.e6. doi: 10.1016/j.ajog.2018.04.002. Epub 2018 Apr 7.
Women with a history of hypertensive disease of pregnancy have increased risks for early mortality from multiple causes. The effect of recurrent hypertensive disease of pregnancy on mortality risk and life expectancy is unknown.
We sought to determine whether recurrent hypertensive disease of pregnancy is associated with increased mortality risks.
In this retrospective cohort study, we used birth certificate data to determine the number of pregnancies affected by hypertensive disease of pregnancy for each woman delivering in Utah from 1939 through 2012. We assigned women to 1 of 3 groups based on number of affected pregnancies: 0, 1, or ≥2. Exposed women had ≥1 affected singleton pregnancy and lived in Utah for ≥1 year postpartum. Exposed women were matched 1:2 to unexposed women by age, year of childbirth, and parity. Underlying cause of death was determined from death certificates. Mortality risks by underlying cause of death were compared between exposed and unexposed women as a function of number of affected pregnancies. Cox regressions controlled for infant sex, gestational age, parental education, ethnicity, and marital status.
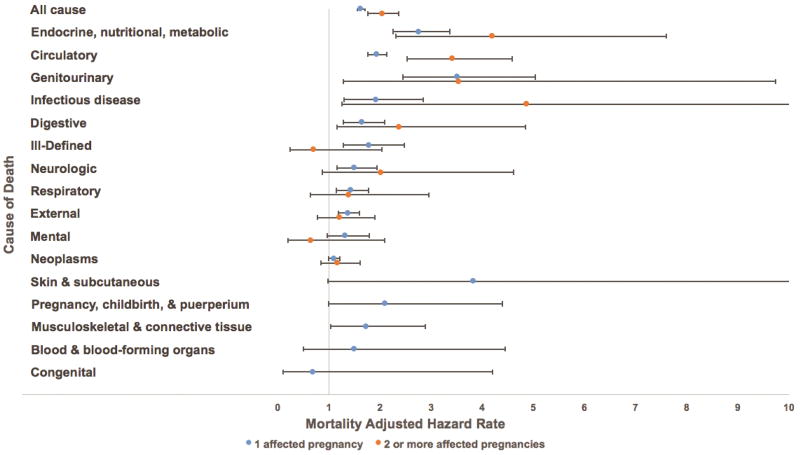
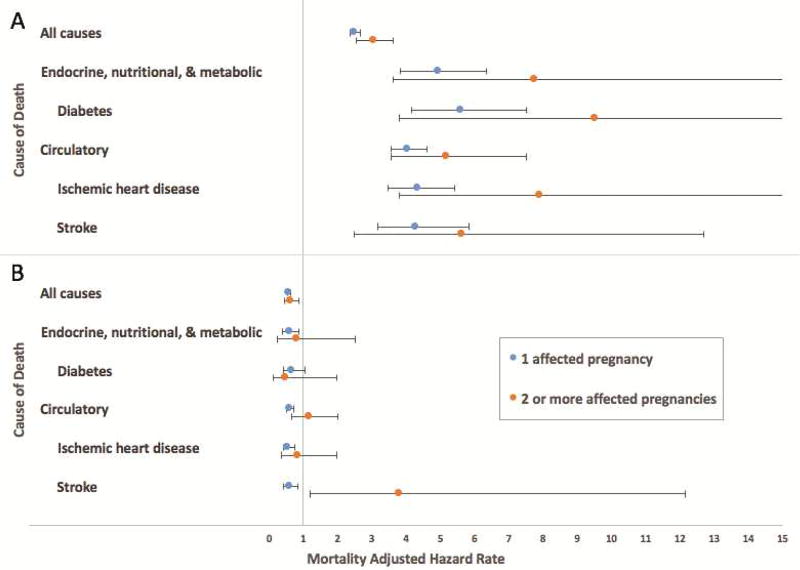
We identified 57,384 women with ≥1 affected pregnancy (49,598 women with 1 affected pregnancy and 7786 women with ≥2 affected pregnancies). These women were matched to 114,768 unexposed women. As of 2016, 11,894 women were deceased: 4722 (8.2%) exposed and 7172 (6.3%) unexposed. Women with ≥2 affected pregnancies had increased mortality from all causes (adjusted hazard ratio, 2.04; 95% confidence interval, 1.76-2.36), diabetes (adjusted hazard ratio, 4.33; 95% confidence interval, 2.21-8.47), ischemic heart disease (adjusted hazard ratio, 3.30; 95% confidence interval, 2.02-5.40), and stroke (adjusted hazard ratio, 5.10; 95% confidence interval, 2.62-9.92). For women whose index pregnancy delivered from 1939 through 1959 (n = 10,488), those with ≥2 affected pregnancies had shorter additional life expectancies than mothers who had only 1 or 0 hypertensive pregnancies (48.92 vs 51.91 vs 55.48 years, respectively).
Hypertensive diseases of pregnancy are associated with excess risks for early all-cause mortality and some cause-specific mortality, and these risks increase further with recurrent disease.
患有妊娠高血压疾病的女性因多种原因导致早期死亡率增加。复发性妊娠高血压疾病对死亡率和预期寿命的影响尚不清楚。
我们旨在确定复发性妊娠高血压疾病是否与更高的死亡率风险相关。
在这项回顾性队列研究中,我们使用出生证明数据确定了 1939 年至 2012 年期间在犹他州分娩的每位女性的妊娠高血压疾病受影响的妊娠次数。我们根据受影响的妊娠次数将女性分为 3 组之一:0、1 或≥2。暴露组女性有≥1 次受影响的单胎妊娠,并在产后至少在犹他州居住 1 年。暴露组女性按年龄、分娩年份和产次与未暴露组女性 1:2 匹配。死亡原因根据死亡证明确定。根据受影响的妊娠次数,比较暴露组和未暴露组女性的不同死因的死亡率风险。Cox 回归控制了婴儿性别、胎龄、父母教育、种族和婚姻状况。
我们确定了 57384 名患有≥1 次受影响妊娠的女性(49598 名患有 1 次受影响妊娠,7786 名患有≥2 次受影响妊娠)。这些女性与 114768 名未暴露的女性相匹配。截至 2016 年,有 11894 名女性死亡:4722 名(8.2%)暴露和 7172 名(6.3%)未暴露。患有≥2 次受影响妊娠的女性因各种原因(调整后的危险比,2.04;95%置信区间,1.76-2.36)、糖尿病(调整后的危险比,4.33;95%置信区间,2.21-8.47)、缺血性心脏病(调整后的危险比,3.30;95%置信区间,2.02-5.40)和中风(调整后的危险比,5.10;95%置信区间,2.62-9.92)的死亡率更高。对于索引妊娠从 1939 年至 1959 年分娩的女性(n=10488),患有≥2 次受影响妊娠的女性的预期寿命比仅患有 1 次或 0 次高血压妊娠的母亲更短(分别为 48.92 岁、51.91 岁和 55.48 岁)。
妊娠高血压疾病与早期全因死亡率和某些病因特异性死亡率的风险增加相关,并且随着疾病的复发,这些风险进一步增加。