Department of Surgery and Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan.
College of Medicine, National Taiwan University, Taipei, Taiwan.
BMC Cancer. 2018 Apr 10;18(1):401. doi: 10.1186/s12885-018-4292-y.
Research has revealed that angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) may prevent cancers such as hepatocellular carcinoma (HCC). The comparative chemopreventive effects of ACEIs and ARBs in high-risk populations with hepatitis B virus (HBV) or hepatitis C virus (HCV) infection have yet to be investigated.
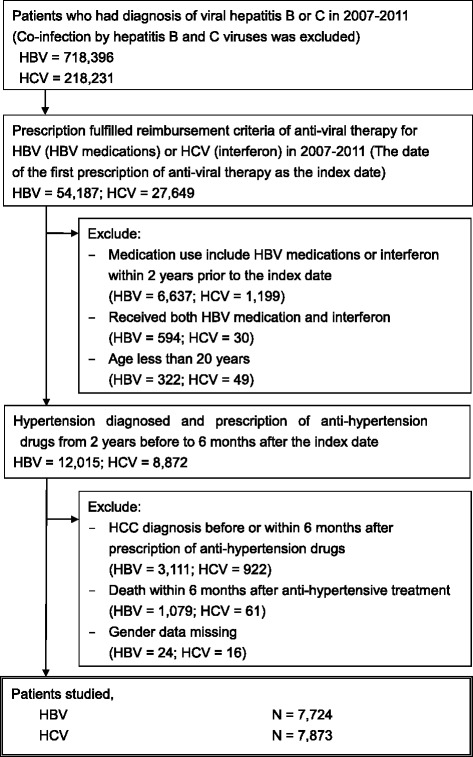
From 2005 to 2014, high-risk HBV and HCV cohorts of hypertensive patients without HCC history were recruited from three linked national databases of Taiwan, and were classified into two groups based on the ACEI or ARB exposure within the initial six months after initiating antiviral agent. Intergroup differences in clinical characteristics and duration of drug exposure within study period were evaluated. HCC-free survival was compared using the log-rank test. Multivariate Cox regression including time-dependent variables for the use of ACEIs or ARBs and other medications was applied to adjust for confounders.
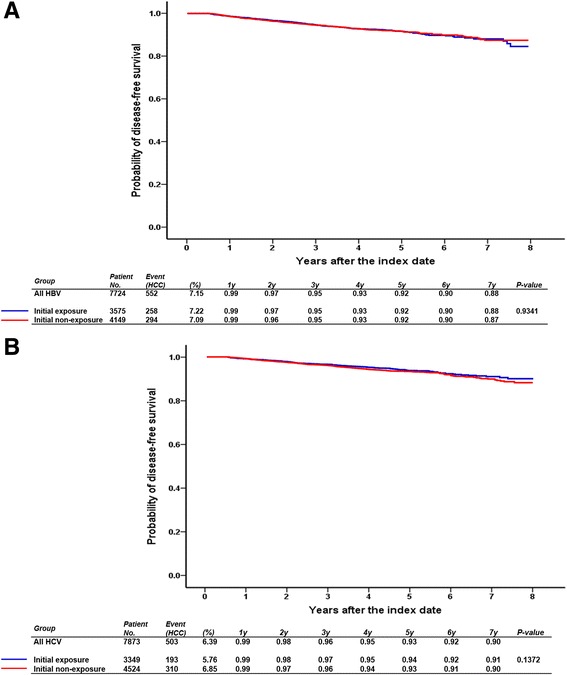
Among the 7724 patients with HBV and 7873 with HCV, 46.3% and 42.5%, respectively, had an initial exposure to ACEIs or ARBs. The median durations of exposure were 36.4 and 38.9 months for the HBV and HCV cohorts, respectively. The median durations of ACEI or ARB use during study period between initial exposure and nonexposure groups were 41.8 vs. 18.3 months and 46.4 vs. 22.7 months for the HBV and HCV cohorts, respectively. No significant difference was observed in HCC risk within 7 years between the initial exposure and non-exposure groups. After adjustment for comorbidities, namely liver cirrhosis, diabetes mellitus (DM), and hyperlipidemia, and medications, namely aspirin, metformin, and statins, the hazard ratios (HRs) for ACEI or ARB exposure for HCC risk were 0.97 (95% confidence interval [CI]: 0.81-1.16) and 0.96 (0.80-1.16) in the HBV and HCV cohorts, respectively. In the HCV cohort, the increased HCC risk was associated with ACEI or ARB use in patients without cirrhosis, DM, and hyperlipidemia (HR: 4.53, 95% CI: 1.46-14.1).
Compared with other significant risk and protective factors for HCC, ACEI or ARB use in the HBV and HCV cohorts was not associated with adequate protective effectiveness under standard dosages and may not be completely safe.
研究表明,血管紧张素转换酶抑制剂(ACEIs)和血管紧张素 II 受体阻滞剂(ARBs)可能预防肝癌(HCC)等癌症。然而,乙型肝炎病毒(HBV)或丙型肝炎病毒(HCV)感染高危人群中 ACEIs 和 ARBs 的比较化学预防效果仍有待研究。
2005 年至 2014 年,从台湾的三个相关国家数据库中招募了没有 HCC 病史的高血压高危 HBV 和 HCV 队列患者,并根据抗病毒药物治疗开始后最初 6 个月内 ACEI 或 ARB 的暴露情况将其分为两组。评估了研究期间两组之间的临床特征和药物暴露时间的差异。使用对数秩检验比较 HCC 无复发生存率。应用包括 ACEIs 或 ARBs 以及其他药物使用时间依赖性变量的多变量 Cox 回归来调整混杂因素。
在 7724 例 HBV 和 7873 例 HCV 患者中,分别有 46.3%和 42.5%的患者最初使用了 ACEIs 或 ARBs。HBV 和 HCV 队列的暴露中位数分别为 36.4 和 38.9 个月。在初始暴露组和非暴露组中,研究期间 ACEI 或 ARB 使用的中位数持续时间分别为 41.8 个月和 18.3 个月和 46.4 个月和 22.7 个月。HBV 和 HCV 队列中,在 7 年内,初始暴露组和非暴露组的 HCC 风险无显著差异。在调整了肝硬化、糖尿病(DM)、高脂血症和阿司匹林、二甲双胍、他汀类药物等共病和药物后,HBV 和 HCV 队列中 ACEI 或 ARB 暴露的 HCC 风险的危险比(HR)分别为 0.97(95%置信区间[CI]:0.81-1.16)和 0.96(0.80-1.16)。在 HCV 队列中,与无肝硬化、DM 和高脂血症的患者相比,ACEI 或 ARB 的使用与 HCC 风险增加相关(HR:4.53,95%CI:1.46-14.1)。
与 HCC 的其他重要风险和保护因素相比,HBV 和 HCV 队列中 ACEI 或 ARB 的使用在标准剂量下与足够的保护效果无关,并且可能不完全安全。