Byrne B E, Vincent C A, Faiz O D
Imperial Patient Safety Translational Research Centre, Imperial College London, London, UK.
Bristol Centre for Surgical Research, Population Health Sciences, Bristol Medical School, University of Bristol, Canynge Hall, 39 Whatley Road, Bristol, BS8 2PS, UK.
World J Surg. 2018 Oct;42(10):3422-3431. doi: 10.1007/s00268-018-4615-9.
Laparoscopic colorectal cancer surgery has developed from unproven technique to mainstay of treatment. This study examined the application and relative outcomes of laparoscopic and open colorectal cancer surgery over time, as laparoscopic uptake and experience have grown.
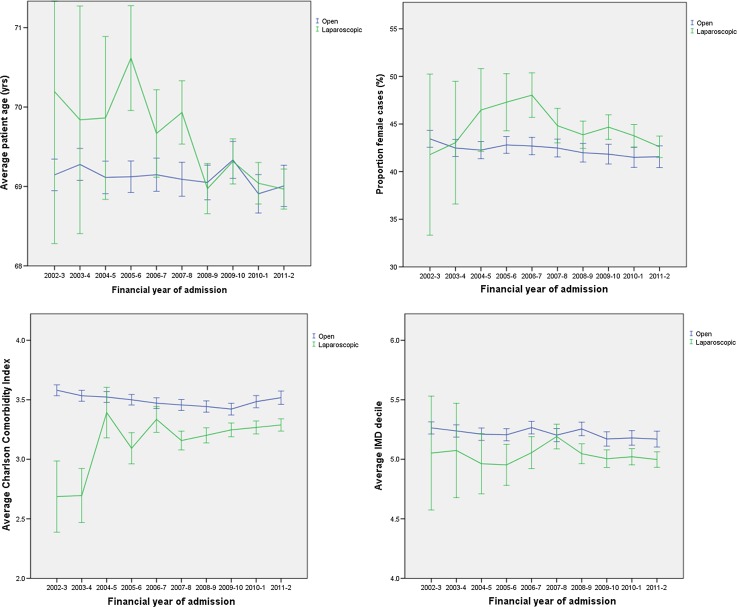
Adults undergoing elective laparoscopic and open colorectal cancer surgery in the English NHS during 2002-2012 were included. Age, sex, Charlson Comorbidity Index and Index of Multiple Deprivation were compared over time. Post-operative 30-day mortality, length of stay, failure to rescue reoperation and the associated mortality rate were examined.
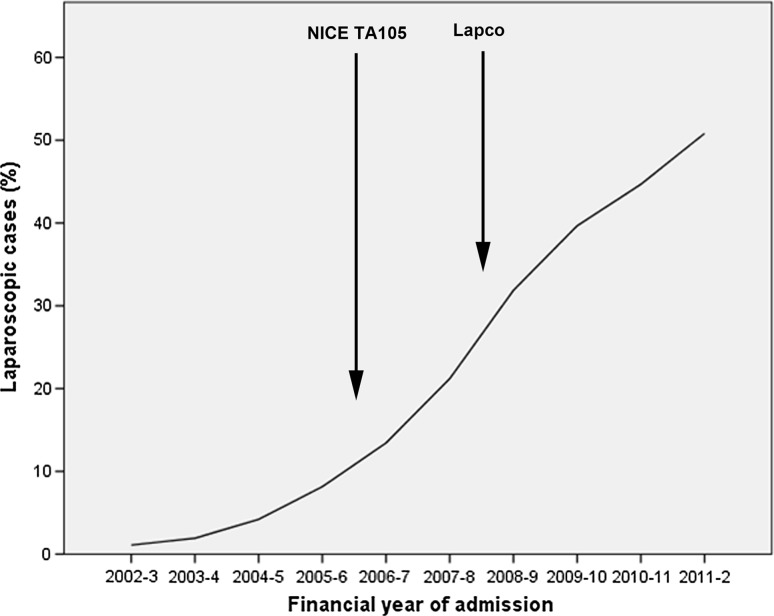
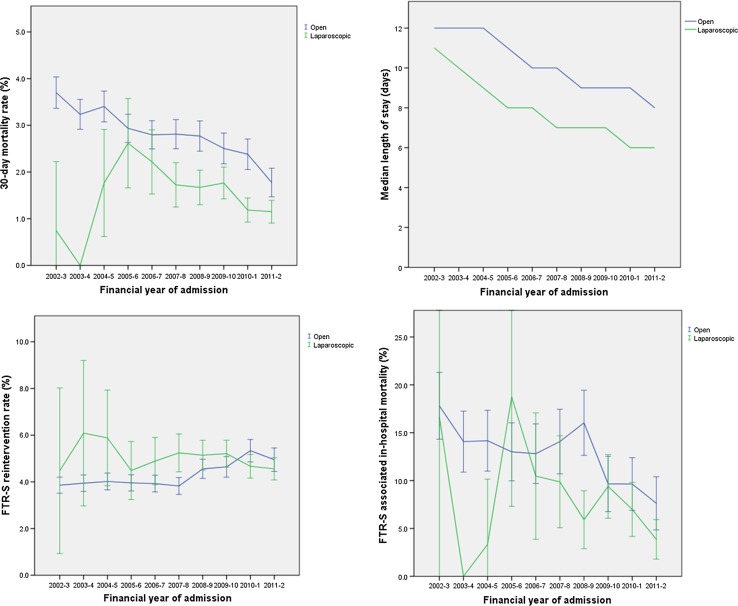
Laparoscopy rates rose from 1.1 to 50.8%. Patients undergoing laparoscopic surgery had lower comorbidity by 0.24 points (95% confidence intervals (CI) 0.20-0.27) and lower socioeconomic deprivation by 0.16 deciles (95% CI 0.12-0.20) than those having open procedures. Overall mortality fell by 48.0% from 2002-2003 to 2011-2002 and was 37.8% lower after laparoscopic surgery. Length of stay and mortality after surgical re-intervention also fell. However, re-intervention rates were higher after laparoscopic procedures by 7.8% (95% CI 0.9-15.2%).
There was clear and persistent inequality in the application of laparoscopic colorectal cancer surgery during this study. Further work must explore and remedy inequalities to maximise patient benefit. Higher re-intervention rates after laparoscopy are unexplained and differ from randomized controlled trials. This may reflect differences in surgeons and practice between research and usual care settings and should be further investigated.
腹腔镜结直肠癌手术已从未经证实的技术发展成为主要治疗手段。随着腹腔镜手术的应用增加和经验积累,本研究探讨了腹腔镜和开放结直肠癌手术随时间推移的应用情况及相关结果。
纳入2002年至2012年在英国国民健康服务体系(NHS)接受择期腹腔镜和开放结直肠癌手术的成年人。比较不同时间点的年龄、性别、查尔森合并症指数和多重剥夺指数。检查术后30天死亡率、住院时间、挽救性再次手术失败率及相关死亡率。
腹腔镜手术率从1.1%升至50.8%。与接受开放手术的患者相比,接受腹腔镜手术的患者合并症低0.24分(95%置信区间(CI)0.20 - 0.27),社会经济剥夺程度低0.16十分位数(95%CI 0.12 - 0.20)。总体死亡率从2002 - 2003年至2011 - 2012年下降了48.0%,腹腔镜手术后降低了37.8%。手术再次干预后的住院时间和死亡率也有所下降。然而,腹腔镜手术后的再次干预率高7.8%(95%CI 0.9 - 15.2%)。
在本研究期间,腹腔镜结直肠癌手术的应用存在明显且持续的不平等现象。必须进一步开展工作以探索并纠正不平等现象,从而使患者受益最大化。腹腔镜手术后较高的再次干预率原因不明,且与随机对照试验结果不同。这可能反映了研究与常规医疗环境中外科医生及操作的差异,应进一步研究。