Wilson Parker C, Kashgarian Michael, Moeckel Gilbert
Department of Pathology, Yale University School of Medicine, New Haven, CT, USA.
Clin Kidney J. 2018 Apr;11(2):207-218. doi: 10.1093/ckj/sfx093. Epub 2017 Aug 31.
This study examines the effect of interstitial inflammation and interstitial fibrosis and tubular atrophy on renal survival in lupus nephritis.
Baseline characteristics, initial ( = 301) and repeat biopsies ( = 94) and clinical outcomes for patients with biopsy-proven lupus nephritis from 1998 to 2014 were retrospectively collected from the medical record. Clinical and morphologic variables were evaluated using a Cox proportional hazards model and multiple imputation to address missing data. Renal survival was defined as the time from initial biopsy to end-stage renal disease [estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m], dialysis or transplant.
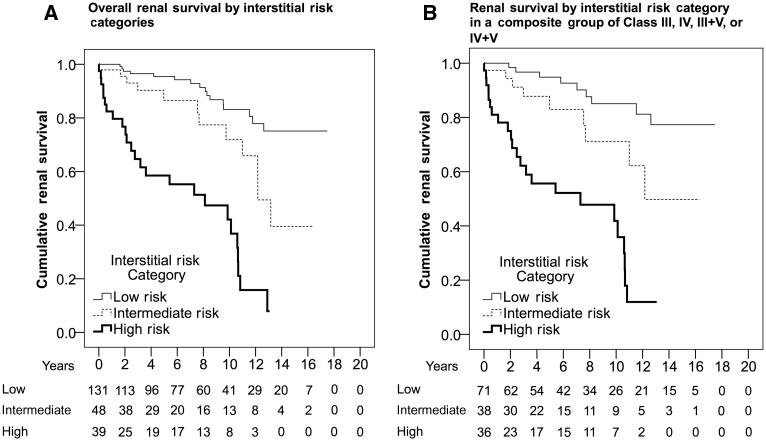
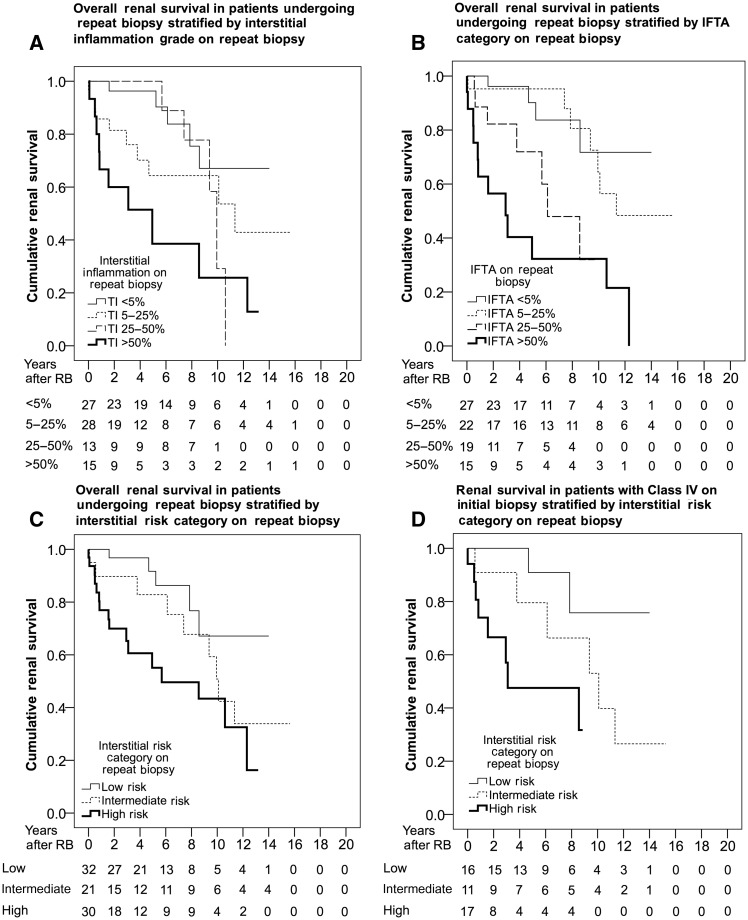
A total of 218 patients had follow-up and Class IV had worse renal survival, especially in patients with active and chronic glomerular lesions {relative to non-IV; Class IV-A: hazard ratio [HR] 0.92 [95% confidence interval (CI) 0.41-2.04], Class IV-AC: HR 5.02 [95% CI 2.70-9.36]}. Interstitial inflammation grade [relative to interstitial inflammation <5%; interstitial inflammation 5-25%: HR 2.36 (95% CI 1.13-4.91), interstitial inflammation 25-50%: HR 3.84 (95% CI 1.53-9.62), interstitial inflammation >50%: HR 7.67 (95% CI 3.75-15.67)] and increased interstitial fibrosis and tubular atrophy (IFTA) category [relative to IFTA <5%; IFTA 5-25%: HR 3.93 (95% CI 1.58-9.75), IFTA 25-50%: HR 4.01 (95% CI 1.37-11.70), IFTA >50%: HR 13.99 (95% CI 4.91-39.83)] predicted worse renal survival among all patients and those with Class IV on initial and repeat biopsy ( = 94) in a dose-dependent manner. Interstitial inflammation grade and IFTA category were significant predictors of renal survival in a multivariable model adjusted for age, gender, race, ethnicity and serum creatinine.
Interstitial inflammation and IFTA independently affect renal survival and grading these lesions stratifies risk within the International Society of Nephrology and Renal Pathology Society classification of lupus nephritis.
本研究探讨间质性炎症、间质纤维化和肾小管萎缩对狼疮性肾炎患者肾脏存活的影响。
回顾性收集1998年至2014年经活检证实为狼疮性肾炎患者的基线特征、初次活检(n = 301)和重复活检(n = 94)以及临床结局。使用Cox比例风险模型和多重填补法评估临床和形态学变量以处理缺失数据。肾脏存活定义为从初次活检至终末期肾病[估计肾小球滤过率(eGFR)<15 mL/min/1.73 m²]、透析或移植的时间。
共有218例患者接受随访,IV级患者的肾脏存活率较低,尤其是伴有活动性和慢性肾小球病变的患者{相对于非IV级;IV - A级:风险比[HR] 0.92 [95%置信区间(CI)0.41 - 2.04],IV - AC级:HR 5.02 [95% CI 2.70 - 9.36]}。在所有患者以及初次和重复活检为IV级的患者(n = 94)中,间质性炎症分级[相对于间质性炎症<5%;间质性炎症5 - 25%:HR 2.36(95% CI 1.13 - 4.91),间质性炎症25 - 50%:HR 3.84(95% CI 1.53 - 9.62),间质性炎症>50%:HR 7.67(95% CI 3.75 - 15.67)]以及间质纤维化和肾小管萎缩(IFTA)程度增加[相对于IFTA<5%;IFTA 5 - 25%:HR 3.93(95% CI 1.58 - 9.75),IFTA 25 - 50%:HR 4.01(95% CI 1.37 - 11.70),IFTA>50%:HR 13.99(95% CI 4.91 - 39.83)]以剂量依赖方式预示着较差的肾脏存活率。在调整了年龄、性别、种族、民族和血清肌酐的多变量模型中,间质性炎症分级和IFTA程度是肾脏存活的显著预测因素。
间质性炎症和IFTA独立影响肾脏存活,在国际肾脏病学会和肾脏病理学会的狼疮性肾炎分类中,对这些病变进行分级可对风险进行分层。