Center for Cardiovascular Research, Charité Universitaetsmedizin Berlin, Berlin, Germany.
Department of Vascular Surgery, University Hospital Zurich, Zurich, Switzerland.
PLoS One. 2018 Apr 12;13(4):e0195828. doi: 10.1371/journal.pone.0195828. eCollection 2018.
The use of iodine-based contrast agents entails the risk of contrast induced nephropathy (CIN). Radiocontrast agents elicit the third most common cause of nephropathy among hospitalized patients, accounting for 11-12% of cases. CIN is connected with clinically significant consequences, including increased morbidity, prolonged hospitalization, increased risk of complications, potential need for dialysis, and increased mortality rate. The number of in-hospital examinations using iodine-based contrast media has been significantly increasing over the last decade. In order to protect patients from possible complications of such examinations, new biomarkers are needed that are able to predict a risk of contrast-induced nephropathy. Urinary and plasma cyclic guanosine monophosphate (cGMP) concentrations are influenced by renal function. Urinary cGMP is primarily of renal cellular origin. Therefore, we assessed if urinary cGMP concentration may predict major adverse renal events (MARE) after contrast media exposure during coronary angiography.
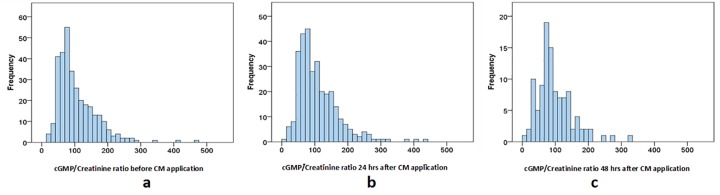
Urine samples were prospectively collected from non-randomized consecutive patients with either diabetes or preexisting impaired kidney function receiving intra-arterial contrast medium (CM) for emergent or elective coronary angiography at the Charité Campus Mitte, University Hospital Berlin. Urinary cGMP concentration in spot urine was analyzed 24 hours after CM exposure. Patients were followed up over 90 days for occurrence of death, initiation of dialysis, doubling of plasma creatinine concentration or MARE.
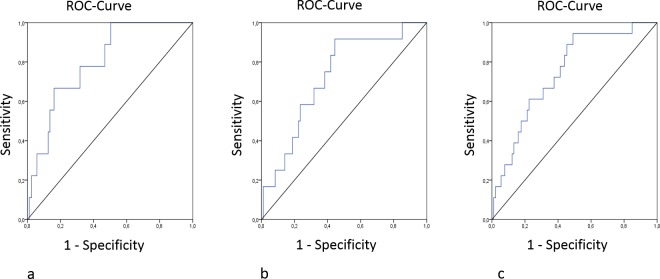
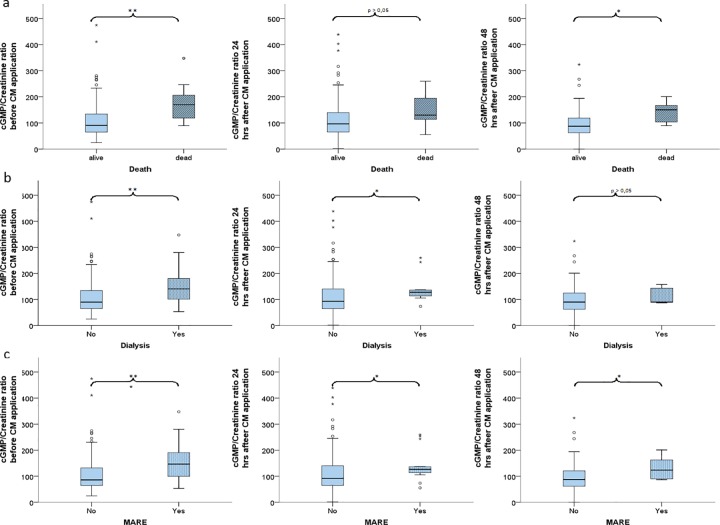
In total, 289 consecutive patients were included into the study. Urine cGMP/creatinine ratio 24 hours before CM exposure expressed as mean±SD was predictive for the need of dialysis (no dialysis: 89.77±92.85 μM/mM, n = 277; need for dialysis: 140.3±82.90 μM/mM, n = 12, p = 0.008), death (no death during follow-up: 90.60±92.50 μM/mM, n = 280; death during follow-up: 169.88±81.52 μM/mM, n = 9; p = 0.002), and the composite endpoint MARE (no MARE: 86.02±93.17 μM/mM, n = 271; MARE: 146.64±74.68 μM/mM, n = 18, p<0.001) during the follow-up of 90 days after contrast media application. cGMP/creatinine ratio stayed significantly increased at values exceeding 120 μM/mM in patients who developed MARE, required dialysis or died.
Urinary cGMP/creatinine ratio ≥ 120 μM/mM before CM exposure is a promising biomarker for the need of dialysis and all-cause mortality 90 days after CM exposure in patients with preexisting renal impairment or diabetes.
碘造影剂的使用存在造影剂诱导肾病(CIN)的风险。造影剂是导致住院患者发生肾病的第三大常见原因,占 11-12%。CIN 会导致严重的临床后果,包括发病率增加、住院时间延长、并发症风险增加、潜在透析需求增加和死亡率增加。过去十年中,使用碘造影剂的住院检查数量显著增加。为了保护患者免受此类检查的潜在并发症影响,需要新的生物标志物来预测造影剂诱导的肾病风险。尿和血浆环鸟苷酸(cGMP)浓度受肾功能影响。尿 cGMP 主要来源于肾细胞。因此,我们评估了冠状动脉造影时,造影剂暴露后尿 cGMP 浓度是否可预测主要不良肾脏事件(MARE)。
前瞻性收集来自接受动脉内造影剂(CM)的糖尿病或预先存在肾功能不全的非随机连续患者的尿液样本,用于柏林夏洛蒂医科大学 Charité Campus Mitte 的紧急或选择性冠状动脉造影。在 CM 暴露后 24 小时分析尿液 cGMP 浓度。患者在 90 天内随访死亡、开始透析、血肌酐浓度加倍或 MARE 的发生情况。
共纳入 289 例连续患者。CM 暴露前 24 小时尿 cGMP/肌酐比值的平均值±标准差可预测需要透析的情况(无透析:89.77±92.85 μM/mM,n = 277;需要透析:140.3±82.90 μM/mM,n = 12,p = 0.008)、死亡(随访期间无死亡:90.60±92.50 μM/mM,n = 280;随访期间死亡:169.88±81.52 μM/mM,n = 9;p = 0.002)以及复合终点 MARE(无 MARE:86.02±93.17 μM/mM,n = 271;MARE:146.64±74.68 μM/mM,n = 18,p<0.001)。在 CM 应用后 90 天的随访期间,发生 MARE、需要透析或死亡的患者的 cGMP/肌酐比值持续显著升高,超过 120 μM/mM。
CM 暴露前尿 cGMP/肌酐比值≥120 μM/mM 是预测肾功能不全或糖尿病患者 CM 暴露后 90 天透析和全因死亡率的有前途的生物标志物。