School of Medicine, Western Sydney University, Locked Bag 1797, Penrith NSW, Sydney, 2751, Australia.
School of Science and Health, Western Sydney University, Locked Bag 1797, Penrith NSW, Sydney, 2571, Australia.
BMC Cancer. 2018 Apr 12;18(1):410. doi: 10.1186/s12885-018-4185-0.
Although acute oxaliplatin-induced neuropathy (OXIPN) is frequently regarded to be transient, recent studies have reported prolongation of infusion times, dose reduction and treatment cessation following the first dose of oxaliplatin in quarter of patients. Acute OXIPN is also a well-established risk factor for chronic neuropathy. However, there is underreporting of these parameters during the acute phase (≤ 14 days). This paper systematically reviews the incidence of acute OXIPN and its impact on treatment in the first cycle.
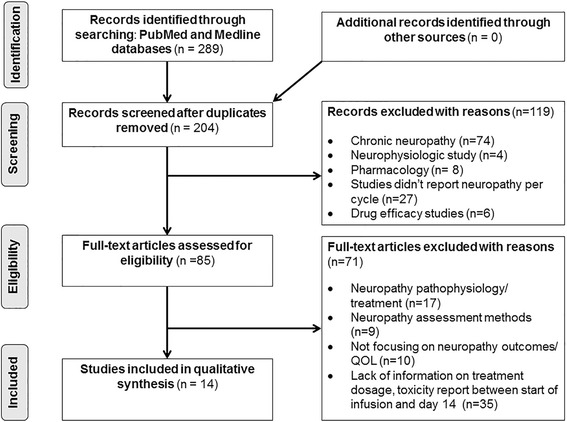
A systematic literature search was performed using PubMed and Medline. Published original articles were included if they described details about prevalence of oxaliplatin-induced acute neuropathy.
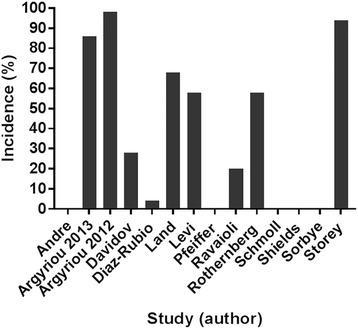
Fourteen studies, comprised of 6211 patients were evaluated. The majority of patients were treated with oxaliplatin in combination with leucovorin and fluorouracil (FOLFOX). Most studies used the National Cancer Institute Common Toxicity Criteria to assess acute neuropathy. Acute neuropathy (Grades 1-4) was the most common event with prevalence ranging from 4-98%, followed by haematological (1.4-81%) and gastrointestinal (1.2-67%) toxicities, respectively. Drug regimens, starting dose of oxaliplatin and neuropathy assessment tools varied across studies. In addition, moderate to severe toxicities were common in patients that received a large dose of oxaliplatin (> 85 mg/m) and/ or combined drugs. The majority of studies did not report the factors affecting acute neuropathy namely the range (minimal) doses required to evoke acute neuropathy, patient and clinical risk factors. In addition, there was no systematic reporting of the number of patients subjected to prolonged infusion, dose reduction, treatment delay and treatment cessation during the acute phase.
Despite the heterogeneity of studies regarding oxaliplatin starting dose, drug regimen, neuropathy assessment tools and study design, a large number of patients developed acute neuropathy. To develop a better preventive and therapeutic guideline for acute/chronic neuropathy, a prospective study should be conducted in a large cohort of patients in relation to drug regimen, starting/ranges (minimal) of doses producing acute neuropathy, treatment compliance, patient and clinical risk factors using a standardised neuropathy assessment tool.
尽管急性奥沙利铂诱导的神经病(OXIPN)通常被认为是短暂的,但最近的研究报告称,在四分之一的患者中,奥沙利铂的首次剂量后,输注时间延长、剂量减少和治疗停止。急性 OXIPN 也是慢性神经病的一个既定危险因素。然而,在急性阶段(≤14 天),这些参数的报告不足。本文系统回顾了第一周期中急性 OXIPN 的发生率及其对治疗的影响。
使用 PubMed 和 Medline 进行系统文献检索。如果原始文章详细描述了奥沙利铂诱导的急性神经病的流行情况,则将其包括在内。
评估了 14 项研究,共包括 6211 名患者。大多数患者接受奥沙利铂联合亚叶酸和氟尿嘧啶(FOLFOX)治疗。大多数研究使用国家癌症研究所常见毒性标准评估急性神经病。急性神经病(1-4 级)是最常见的事件,发生率为 4-98%,其次是血液学毒性(1.4-81%)和胃肠道毒性(1.2-67%)。药物方案、奥沙利铂起始剂量和神经病评估工具在不同研究中有所不同。此外,接受大剂量奥沙利铂(>85mg/m)和/或联合药物治疗的患者中,中度至重度毒性很常见。大多数研究未报告影响急性神经病的因素,即引起急性神经病所需的最小剂量范围、患者和临床危险因素。此外,在急性阶段,没有系统报告需要延长输注、减少剂量、延迟治疗和停止治疗的患者数量。
尽管关于奥沙利铂起始剂量、药物方案、神经病评估工具和研究设计的研究存在异质性,但大量患者出现了急性神经病。为了制定更好的急性/慢性神经病预防和治疗指南,应在大样本患者队列中进行前瞻性研究,研究内容涉及药物方案、引起急性神经病的起始/最小剂量范围、治疗依从性、患者和临床危险因素,并使用标准化神经病评估工具。