Wright Henry, Wright Tamara, Pohlig Ryan T, Kasner Scott E, Raser-Schramm Jonathan, Reisman Darcy
Department of Physical Therapy, University of Delaware, Newark, DE, 19713, USA.
Biostatistics Core Facility, University of Delaware, Newark, DE, 19713, USA.
BMC Neurol. 2018 Apr 12;18(1):39. doi: 10.1186/s12883-018-1044-1.
Stroke survivors are more physically inactive than even the most sedentary older adults, and low activity is associated with increased risk of recurrent stroke, medical complications, and mortality. We hypothesize that the combination of a fast walking intervention that improves walking capacity, with a step activity monitoring program that facilitates translation of gains from the clinic to the "real-world", would generate greater improvements in real world walking activity than with either intervention alone.
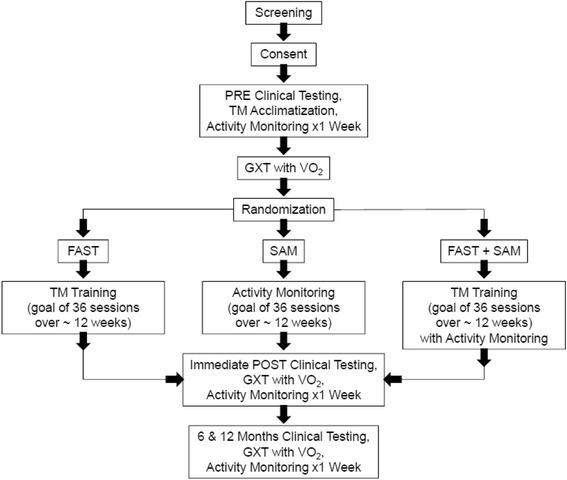
Using a single-blind randomized controlled experimental design, 225 chronic (> 6 months) stroke survivors complete 12 weeks of fast walking training, a step activity monitoring program or a fast walking training + step activity monitoring program. Main eligibility criteria include: chronic ischemic or hemorrhagic stroke (> 6 months post), no evidence of cerebellar stroke, baseline walking speed between 0.3 m/s and 1.0 m/s, and baseline average steps / day < 8000. The primary (steps per day), secondary (self-selected and fastest walking speed, walking endurance, oxygen consumption) and exploratory (vascular events, blood lipids, glucose, blood pressure) outcomes are assessed prior to initiating treatment, after the last treatment and at a 6 and 12-month follow-up. Moderation of the changes in outcomes by baseline characteristics are evaluated to determine for whom the interventions are effective.
Following completion of this study, we will not only understand the efficacy of the interventions and the individuals for which they are effective, we will have the necessary information to design a study investigating the secondary prevention benefits of improved physical activity post-stroke. This study is, therefore, an important step in the development of both rehabilitative and secondary prevention guidelines for persons with stroke.
ClinicalTrials.gov Identifier: NCT02835313 . First Posted: July 18, 2016.
中风幸存者的身体活动水平甚至比久坐不动的老年人还要低,而低活动水平与中风复发、医疗并发症及死亡率增加有关。我们假设,将提高步行能力的快走干预措施与促进从临床获益转化到“现实世界”的步数活动监测计划相结合,相较于单独采用任何一种干预措施,能在现实世界的步行活动中带来更大改善。
采用单盲随机对照实验设计,225名慢性(>6个月)中风幸存者完成12周的快走训练、步数活动监测计划或快走训练+步数活动监测计划。主要纳入标准包括:慢性缺血性或出血性中风(中风后>6个月),无小脑中风证据,基线步行速度在0.3米/秒至1.0米/秒之间,且基线日均步数<8000步。在开始治疗前、最后一次治疗后以及6个月和12个月随访时评估主要(每日步数)、次要(自我选择和最快步行速度、步行耐力、耗氧量)和探索性(血管事件、血脂、血糖、血压)结局。评估基线特征对结局变化的调节作用,以确定干预措施对哪些人有效。
完成本研究后,我们不仅将了解干预措施的疗效及其有效的个体,还将获得必要信息来设计一项研究,调查中风后改善身体活动的二级预防益处。因此,本研究是制定中风患者康复和二级预防指南的重要一步。
ClinicalTrials.gov标识符:NCT02835313。首次发布日期:2016年7月18日。