Unit of Neurology and Unit of Neurorehabilitation, IRCCS Istituto Neurologico Mediterraneo (INM) Neuromed, Via Atinense 18, 86077, Pozzilli, IS, Italy.
Multiple Sclerosis Research Unit, Department of Systems Medicine, Tor Vergata University, Via Montpellier 1, 00133, Rome, Italy.
J Neuroinflammation. 2018 Apr 14;15(1):108. doi: 10.1186/s12974-018-1150-4.
In the early phases of relapsing-remitting multiple sclerosis (RR-MS), a clear correlation between brain lesion load and clinical disability is often lacking, originating the so-called clinico-radiological paradox. Different factors may contribute to such discrepancy. In particular, synaptic plasticity may reduce the clinical expression of brain damage producing enduring enhancement of synaptic strength largely dependent on neurotrophin-induced protein synthesis. Cytokines released by the immune cells during acute inflammation can alter synaptic transmission and plasticity possibly influencing the clinical course of MS. In addition, immune cells may promote brain repair during the post-acute phases, by secreting different growth factors involved in neuronal and oligodendroglial cell survival. Platelet-derived growth factor (PDGF) is a neurotrophic factor that could be particularly involved in clinical recovery. Indeed, PDGF promotes long-term potentiation of synaptic activity in vitro and in MS and could therefore represent a key factor improving the clinical compensation of new brain lesions. The aim of the present study is to explore whether cerebrospinal fluid (CSF) PDGF concentrations at the time of diagnosis may influence the clinical course of RR-MS.
At the time of diagnosis, we measured in 100 consecutive early MS patients the CSF concentrations of PDGF, of the main pro- and anti-inflammatory cytokines, and of reliable markers of neuronal damage. Clinical and radiological parameters of disease activity were prospectively collected during follow-up.
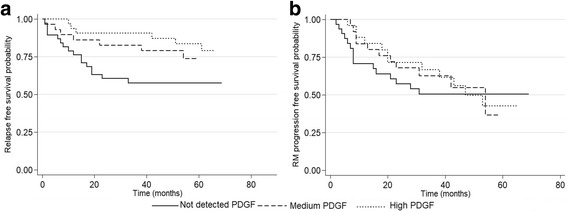
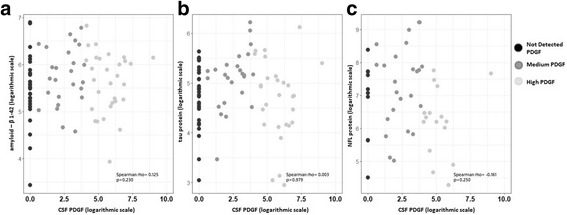
CSF PDGF levels were positively correlated with prolonged relapse-free survival. Radiological markers of disease activity, biochemical markers of neuronal damage, and clinical parameters of disease progression were instead not influenced by PDGF concentrations. Higher CSF PDGF levels were associated with an anti-inflammatory milieu within the central nervous system.
Our results suggest that PDGF could promote a more prolonged relapse-free period during the course of RR-MS, without influencing inflammation reactivation and inflammation-driven neuronal damage and likely enhancing adaptive plasticity.
在复发缓解型多发性硬化症(RR-MS)的早期阶段,脑损伤负荷与临床残疾之间通常缺乏明确的相关性,由此产生了所谓的临床-放射学悖论。不同的因素可能导致这种差异。特别是,突触可塑性可以减少脑损伤的临床表现,产生持久的突触强度增强,这在很大程度上依赖于神经营养因子诱导的蛋白质合成。免疫细胞在急性炎症期间释放的细胞因子可以改变突触传递和可塑性,可能影响 MS 的临床病程。此外,免疫细胞可能通过分泌不同的参与神经元和少突胶质细胞存活的生长因子,在急性后阶段促进脑修复。血小板衍生生长因子(PDGF)是一种神经营养因子,可能特别参与临床恢复。事实上,PDGF 促进体外和 MS 中突触活动的长期增强,因此可以代表改善新脑损伤临床代偿的关键因素。本研究旨在探讨诊断时脑脊液(CSF)PDGF 浓度是否会影响 RR-MS 的临床病程。
在 100 例连续早期 MS 患者中,我们在诊断时测量了 CSF 中 PDGF 的浓度、主要促炎和抗炎细胞因子的浓度以及可靠的神经元损伤标志物的浓度。在随访期间前瞻性收集疾病活动的临床和放射学参数。
CSF PDGF 水平与延长的无复发缓解期呈正相关。疾病活动的放射学标志物、神经元损伤的生化标志物和疾病进展的临床参数不受 PDGF 浓度的影响。更高的 CSF PDGF 水平与中枢神经系统内的抗炎环境有关。
我们的结果表明,PDGF 可能在 RR-MS 病程中促进更长的无复发缓解期,而不影响炎症再激活和炎症驱动的神经元损伤,并可能增强适应性可塑性。