Ranjit Suchitra, Ramanathan Gokul, Ramakrishnan Balasubramaniam, Kissoon Niranjan
Pediatric Intensive Care Unit, Apollo Children's Hospital, Chennai, Tamil Nadu, India.
Department of Medical Education, Apollo Hospitals, Chennai, Tamil Nadu, India.
Indian J Crit Care Med. 2018 Mar;22(3):154-161. doi: 10.4103/ijccm.IJCCM_413_17.
The World Health Organization guidelines provide suggestions on early recognition and treatment of severe dengue (SD); however, mortality in this group can be high and is related both to disease severity and the treatment complications.
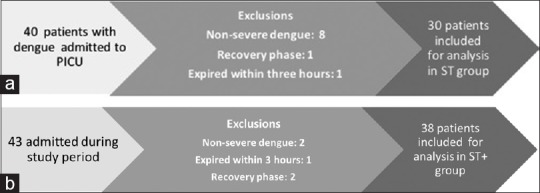
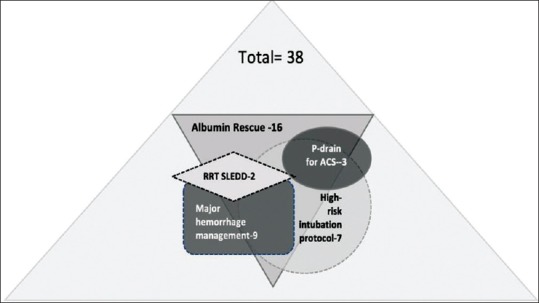
In this prospective observational study, we report our results where standard therapy (ST) was enhanced by Intensive Care Unit (ICU) supportive measures that have proven beneficial in other conditions that share similar pathophysiology of capillary leak and fluid overload. These include early albumin for crystalloid-refractory shock, proactive monitoring for symptomatic abdominal compartment syndrome (ACS), application of a high-risk intubation management protocol, and other therapies. We compared outcomes in a matched retrospective cohort who received ST.
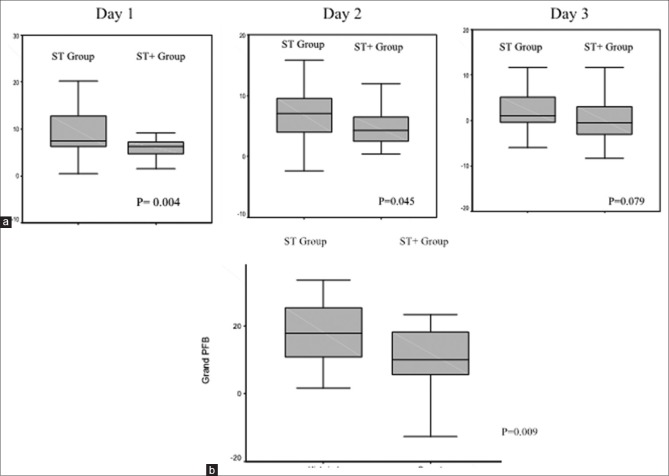
We found improved outcomes using these interventions in patients with the most devastating forms of dengue (ST+ group). We could demonstrate decreased positive fluid balance on days 1-3 and less symptomatic ACS that necessitated invasive percutaneous drainage (7.7% in ST+ group vs. 30% in ST group, = 0.025). Other benefits in ST+ group included lower intubation and positive pressure ventilation requirements (18.4% in ST+ vs. 53.3% in ST, = 0.003), lower incidence of major hemorrhage and acute kidney injury, and reduced pediatric ICU stays and mortality (2.6% in ST+ group vs. 26% in ST group, = 0.004).
Children with SD with refractory shock are at extremely high mortality risk. We describe the proactive application of several targeted ICU supportive interventions in addition to ST and could show that these interventions resulted in decreased resuscitation morbidity and improved outcomes in SD.
世界卫生组织的指南为严重登革热(SD)的早期识别和治疗提供了建议;然而,该组患者的死亡率可能很高,且与疾病严重程度和治疗并发症均有关。
在这项前瞻性观察性研究中,我们报告了通过重症监护病房(ICU)支持措施强化标准治疗(ST)的结果,这些措施已在其他具有类似毛细血管渗漏和液体超负荷病理生理的疾病中证明是有益的。这些措施包括早期使用白蛋白治疗晶体液难治性休克、对有症状的腹腔间隔室综合征(ACS)进行主动监测、应用高风险插管管理方案以及其他治疗方法。我们比较了接受标准治疗的匹配回顾性队列的结局。
我们发现,在最严重形式的登革热患者(ST +组)中使用这些干预措施可改善结局。我们可以证明,在第1 - 3天液体正平衡减少,有症状的ACS减少,从而减少了有创经皮引流的必要性(ST +组为7.7%,ST组为30%,P = 0.025)。ST +组的其他益处包括较低的插管和正压通气需求(ST +组为18.4%,ST组为53.3%,P = 0.003)、较低的大出血和急性肾损伤发生率、缩短儿科ICU住院时间以及降低死亡率(ST +组为2.6%,ST组为26%,P = 0.004)。
患有难治性休克的严重登革热儿童面临极高的死亡风险。我们描述了除标准治疗外积极应用几种有针对性的ICU支持性干预措施,并且可以表明这些干预措施降低了复苏的发病率并改善了严重登革热的结局。