Tweehuysen Lieke, den Broeder Nathan, van Herwaarden Noortje, Joosten Leo A B, van Lent Peter L, Vogl Thomas, van den Hoogen Frank H J, Thurlings Rogier M, den Broeder Alfons A
Department of Rheumatology, Sint Maartenskliniek, Nijmegen, The Netherlands.
Department of Internal Medicine, Radboud University Medical Center, Nijmegen, The Netherlands.
RMD Open. 2018 Apr 9;4(1):e000654. doi: 10.1136/rmdopen-2018-000654. eCollection 2018.
Calprotectin (S100A8/A9) has been correlated with disease activity in rheumatoid arthritis (RA). The aim of this study was to investigate the predictive value of serum calprotectin for clinical response after starting and tapering anti-tumour necrosis factor treatment in RA.
Serum samples and clinical outcomes were derived from two longitudinal RA studies.At baseline (starting or tapering of adalimumab or etanercept), calprotectin levels were determined by ELISA. In the Biologic Individual Optimised Treatment Outcome Prediction (BIO-TOP) study, treatment effect was assessed after 6 months using the European League Against Rheumatism (EULAR) response criteria. In the Dose Reduction Strategies of Subcutaneous TNF Inhibitors (DRESS) study, patients were classified at 18 months as being successfully dose reduced, discontinued or not able to reduce the dose. Area under the receiver operating characteristic curves (AUC) were generated to evaluate the predictive value of calprotectin and logistic prediction models were created to assess its added value.
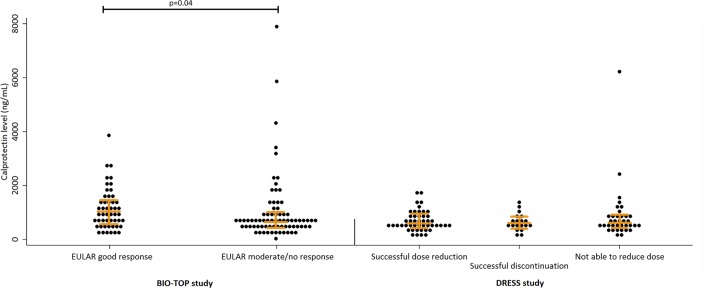
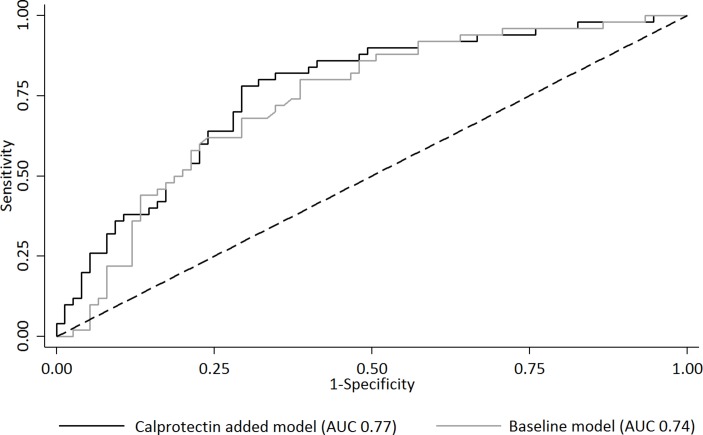
In the BIO-TOP study, calprotectin levels were higher in responders (n=50: 985 ng/mL (p25-p75: 558-1417)) compared with non-responders (n=75: 645 ng/mL (p25-p75: 415-973), p=0.04).AUC for predicting EULAR good response was 0.61 (95% CI 0.50 to 0.71). The prediction model with calprotectin (AUC 0.77, 95% CI 0.68 to 0.85) performed similarly to the baseline model (AUC 0.74, 95% CI 0.65 to 0.82, p=0.29). In the DRESS study, calprotectin levels were similar between the three groups (n=47; n=19; n=36) and calprotectin was not predictive for clinical response after tapering.
Serum calprotectin has some predictive value for clinical response after starting anti-TNF treatment, although it has no added value to other clinical factors. In patients with low disease activity, serum calprotectin is not predictive for clinical response after tapering anti-TNF treatment.
NTR4647 (BIO-TOP study) and NTR3216 (DRESS study); Pre-results.
钙卫蛋白(S100A8/A9)与类风湿关节炎(RA)的疾病活动相关。本研究旨在探讨血清钙卫蛋白对RA患者开始和逐渐减少抗肿瘤坏死因子治疗后临床反应的预测价值。
血清样本和临床结果来自两项RA纵向研究。在基线时(开始或逐渐减少使用阿达木单抗或依那西普),通过酶联免疫吸附测定法测定钙卫蛋白水平。在生物个体化优化治疗结果预测(BIO-TOP)研究中,使用欧洲抗风湿病联盟(EULAR)反应标准在6个月后评估治疗效果。在皮下注射TNF抑制剂剂量减少策略(DRESS)研究中,在18个月时将患者分类为成功减少剂量、停药或无法减少剂量。生成受试者工作特征曲线下面积(AUC)以评估钙卫蛋白的预测价值,并创建逻辑预测模型以评估其附加值。
在BIO-TOP研究中,与无反应者(n = 75:645 ng/mL(第25 - 75百分位数:415 - 973))相比,有反应者(n = 50:985 ng/mL(第25 - 75百分位数:558 - 1417))的钙卫蛋白水平更高(p = 0.04)。预测EULAR良好反应的AUC为0.61(95%置信区间0.50至0.71)。包含钙卫蛋白的预测模型(AUC 0.77,95%置信区间0.68至0.85)与基线模型(AUC 0.74,95%置信区间0.65至0.82,p = 0.29)表现相似。在DRESS研究中,三组(n = 47;n = 19;n = 36)之间的钙卫蛋白水平相似,并且钙卫蛋白对逐渐减少剂量后的临床反应无预测作用。
血清钙卫蛋白对开始抗TNF治疗后的临床反应有一定预测价值,尽管它对其他临床因素无附加值。在疾病活动度低的患者中,血清钙卫蛋白对逐渐减少抗TNF治疗后的临床反应无预测作用。
NTR4647(BIO-TOP研究)和NTR3216(DRESS研究);初步结果。