Division of Environmental Epidemiology, Utrecht University, Institute for Risk Assessment Sciences, Utrecht, The Netherlands.
MRC-PHE Centre for Environment and Health, Department of Epidemiology and Biostatistics, Imperial College London, London, United Kingdom.
Int J Cancer. 2018 Sep 15;143(6):1335-1347. doi: 10.1002/ijc.31536. Epub 2018 Apr 26.
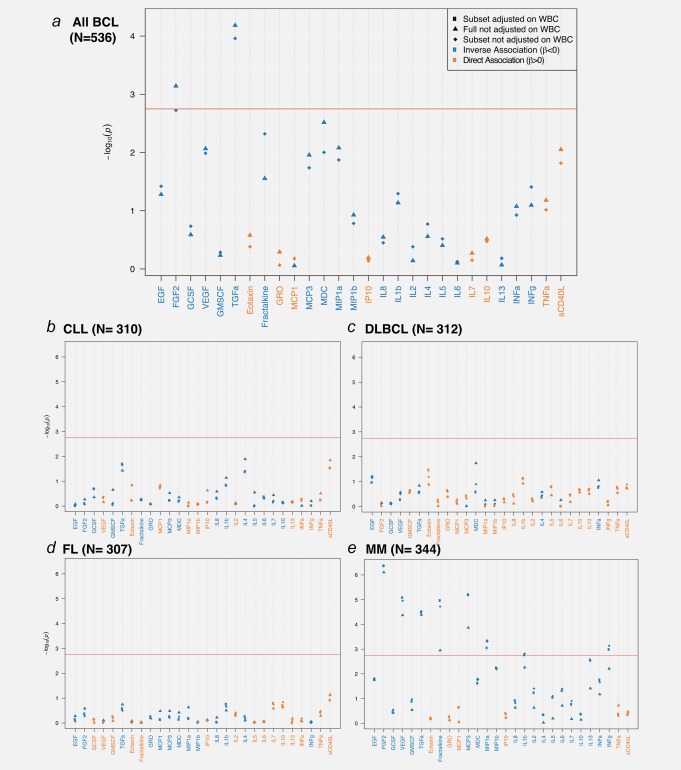
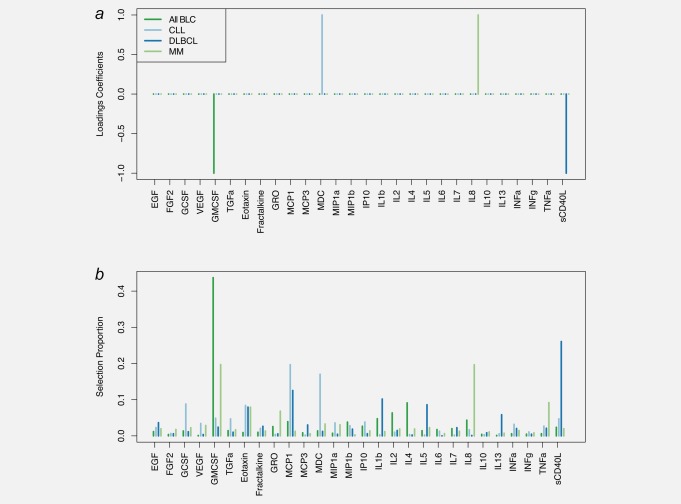
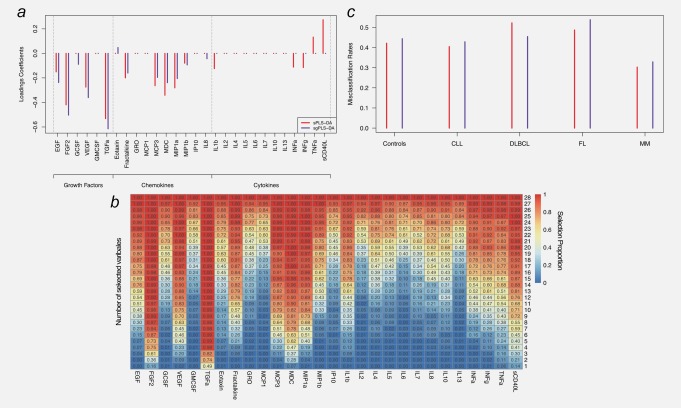
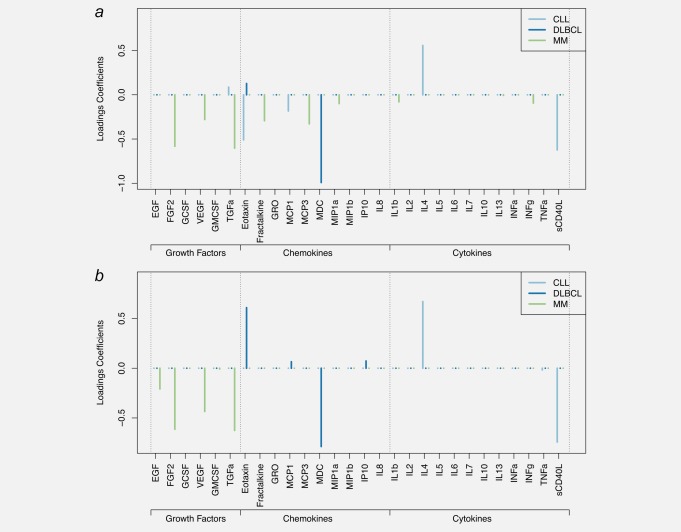
Recent prospective studies have shown that dysregulation of the immune system may precede the development of B-cell lymphomas (BCL) in immunocompetent individuals. However, to date, the studies were restricted to a few immune markers, which were considered separately. Using a nested case-control study within two European prospective cohorts, we measured plasma levels of 28 immune markers in samples collected a median of 6 years before diagnosis (range 2.01-15.97) in 268 incident cases of BCL (including multiple myeloma [MM]) and matched controls. Linear mixed models and partial least square analyses were used to analyze the association between levels of immune marker and the incidence of BCL and its main histological subtypes and to investigate potential biomarkers predictive of the time to diagnosis. Linear mixed model analyses identified associations linking lower levels of fibroblast growth factor-2 (FGF-2 p = 7.2 × 10 ) and transforming growth factor alpha (TGF-α, p = 6.5 × 10 ) and BCL incidence. Analyses stratified by histological subtypes identified inverse associations for MM subtype including FGF-2 (p = 7.8 × 10 ), TGF-α (p = 4.08 × 10 ), fractalkine (p = 1.12 × 10 ), monocyte chemotactic protein-3 (p = 1.36 × 10 ), macrophage inflammatory protein 1-alpha (p = 4.6 × 10 ) and vascular endothelial growth factor (p = 4.23 × 10 ). Our results also provided marginal support for already reported associations between chemokines and diffuse large BCL (DLBCL) and cytokines and chronic lymphocytic leukemia (CLL). Case-only analyses showed that Granulocyte-macrophage colony stimulating factor levels were consistently higher closer to diagnosis, which provides further evidence of its role in tumor progression. In conclusion, our study suggests a role of growth-factors in the incidence of MM and of chemokine and cytokine regulation in DLBCL and CLL.
最近的前瞻性研究表明,免疫系统失调可能先于免疫功能正常个体的 B 细胞淋巴瘤 (BCL) 发展。然而,迄今为止,这些研究仅限于少数被单独考虑的免疫标志物。我们使用两个欧洲前瞻性队列中的嵌套病例对照研究,在 268 例 BCL(包括多发性骨髓瘤 [MM])和匹配对照的诊断前中位数为 6 年(范围 2.01-15.97)的样本中测量了 28 种免疫标志物的血浆水平。线性混合模型和偏最小二乘分析用于分析免疫标志物水平与 BCL 及其主要组织学亚型的发生率之间的关联,并研究潜在的预测诊断时间的生物标志物。线性混合模型分析确定了与较低水平成纤维细胞生长因子 2 (FGF-2,p=7.2×10-7) 和转化生长因子 alpha (TGF-α,p=6.5×10-7) 与 BCL 发生率相关的关联。按组织学亚型分层的分析确定了 MM 亚型的反向关联,包括 FGF-2 (p=7.8×10-7)、TGF-α (p=4.08×10-7)、 fractalkine (p=1.12×10-7)、单核细胞趋化蛋白 3 (p=1.36×10-7)、巨噬细胞炎性蛋白 1-alpha (p=4.6×10-7) 和血管内皮生长因子 (p=4.23×10-7)。我们的结果还为已经报道的趋化因子与弥漫性大 B 细胞淋巴瘤 (DLBCL) 和细胞因子与慢性淋巴细胞白血病 (CLL) 之间的关联提供了边缘支持。仅病例分析表明,粒细胞-巨噬细胞集落刺激因子水平在接近诊断时始终较高,这进一步证明了其在肿瘤进展中的作用。总之,我们的研究表明生长因子在 MM 的发病率、趋化因子和细胞因子在 DLBCL 和 CLL 中的调节中发挥作用。