Working Group on Cardiovascular Magnetic Resonance, Experimental and Clinical Research Center - a joint cooperation between the Charité Medical Faculty and the Max-Delbrück Center for Molecular Medicine, Berlin, Germany.
Department of Cardiology and Nephrology, HELIOS Hospital Berlin-Buch, Berlin, Germany.
ESC Heart Fail. 2018 Aug;5(4):620-629. doi: 10.1002/ehf2.12277. Epub 2018 Apr 19.
This study aims to assess subclinical changes in functional and morphological myocardial magnetic resonance parameters very early into an anthracycline treatment, which may predict subsequent development of anthracycline-induced cardiomyopathy (aCMP).
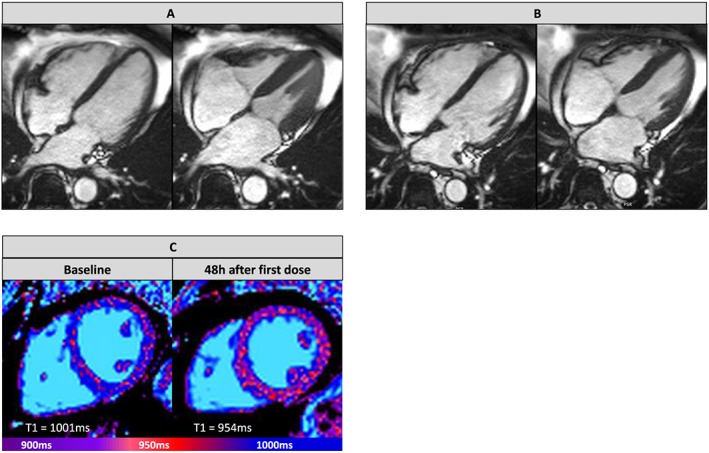
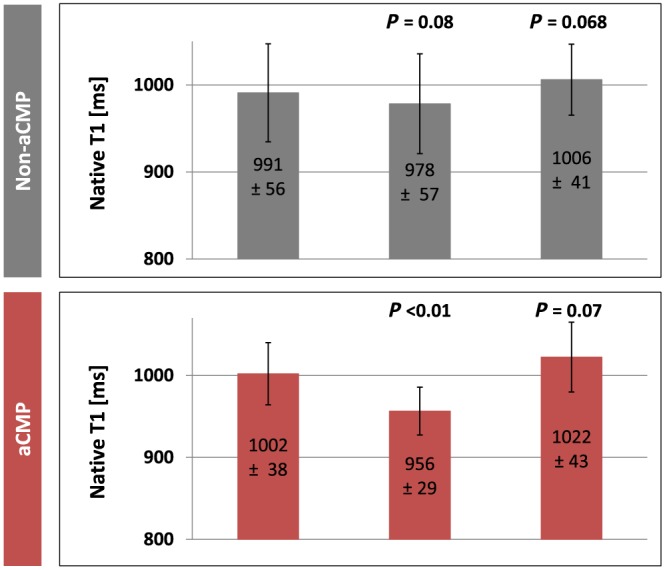
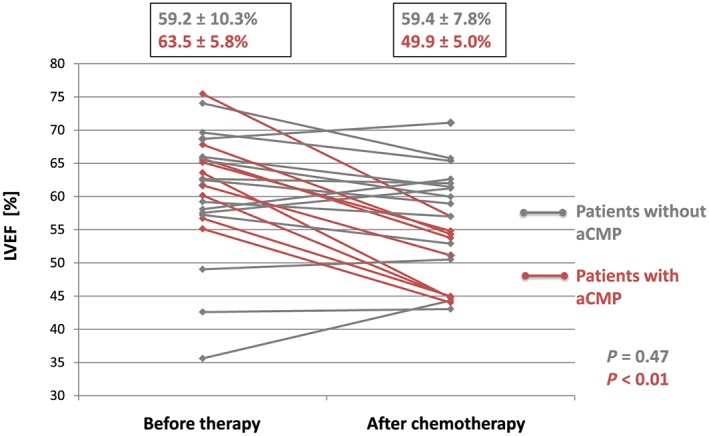
Thirty sarcoma patients with planned anthracycline-based chemotherapy (360-400 mg/m doxorubicin-equivalent) were recruited. Median treatment time was 19.1 ± 2.1 weeks. Enrolled individuals received three cardiovascular magnetic resonance studies (before treatment, 48 h after first anthracycline treatment, and upon completion of treatment). Native T1 mapping (modified Look-Locker inversion recovery 5s(3s)3s), T2 mapping, and extracellular volume maps were acquired in addition to a conventional cardiovascular magnetic resonance with steady-state free precession cine imaging at 1.5 T. Patients were given 0.2 mmol/kg gadoteridol for extracellular volume quantification and late gadolinium enhancement imaging. Development of relevant aCMP was defined as drop of left ventricular ejection fraction (LVEF) by >10%. For analysis, 23 complete data sets were available. Nine patients developed aCMP with LVEF reduction >10% until end of chemotherapy. Baseline LVEF was not different between patients with and without subsequent aCMP. When assessed 48 h after first dose of antracyclines, patients with subsequent aCMP had significantly lower native myocardial T1 times compared with before therapy (1002.0 ± 37.9 vs. 956.5 ± 29.2 ms, P < 0.01) than patients who did not develop aCMP (990.9 ± 56.4 vs. 978.4 ± 57.4 ms, P > 0.05). Patients with aCMP had decreased left ventricular mass upon completion of therapy (86.9 ± 24.5 vs. 81.1 ± 22.3 g; P = 0.02), while patients without aCMP did not show a change in left ventricular mass (81.8 ± 21.0 vs. 79.2 ± 18.1 g; P > 0.05). No patient developed new myocardial scars or compact myocardial fibrosis under chemotherapy.
Early decrease of T1 times 48 h after first treatment with anthracyclines can predict the development of subsequent aCMP after completion of chemotherapy.
本研究旨在评估蒽环类药物治疗早期功能性和形态学心肌磁共振参数的亚临床变化,这些变化可能预测随后发生的蒽环类药物诱导的心肌病(aCMP)。
招募了 30 名计划接受基于蒽环类药物化疗(360-400mg/m 多柔比星等效剂量)的肉瘤患者。中位治疗时间为 19.1±2.1 周。入组患者接受了 3 次心血管磁共振研究(治疗前、首次蒽环类药物治疗后 48 小时和治疗结束时)。除了在 1.5T 上使用稳态自由进动电影成像获得常规心血管磁共振外,还获得了 native T1 映射(改良 Look-Locker 反转恢复 5s(3s)3s)、T2 映射和细胞外容积图。为了进行细胞外容积定量和晚期钆增强成像,患者给予 0.2mmol/kg 钆特醇。发展为相关 aCMP 的定义为左心室射血分数(LVEF)下降>10%。对于分析,有 23 个完整数据集可用。9 名患者发生了 aCMP,LVEF 下降>10%,直至化疗结束。有和没有随后发生 aCMP 的患者之间的基线 LVEF 没有差异。在首次蒽环类药物治疗后 48 小时评估时,与治疗前相比,随后发生 aCMP 的患者的 native 心肌 T1 时间明显降低(1002.0±37.9 与 956.5±29.2ms,P<0.01),而未发生 aCMP 的患者则没有(990.9±56.4 与 978.4±57.4ms,P>0.05)。在完成治疗时,发生 aCMP 的患者左心室质量减少(86.9±24.5 与 81.1±22.3g;P=0.02),而未发生 aCMP 的患者左心室质量没有变化(81.8±21.0 与 79.2±18.1g;P>0.05)。在化疗期间,没有患者出现新的心肌疤痕或致密心肌纤维化。
首次接受蒽环类药物治疗后 48 小时 T1 时间的早期降低可预测化疗后随后发生的 aCMP。