Division of Nephrology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Excellence center for Critical Care Nephrology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand.
Crit Care. 2018 Apr 19;22(1):101. doi: 10.1186/s13054-018-2021-1.
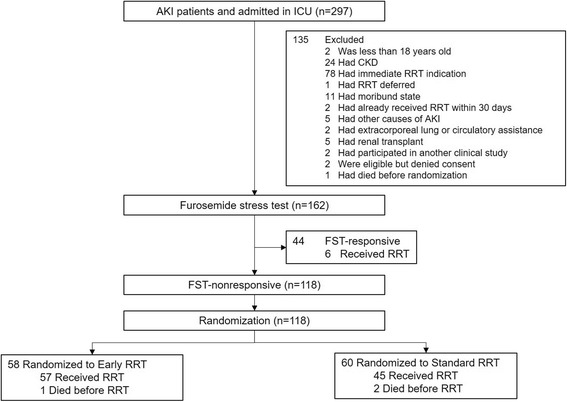
The timing of initiation of renal replacement therapy (RRT) in severe acute kidney injury (AKI) remains controversial, with early initiation resulting in unnecessary therapy for some patients while expectant therapy may delay RRT for other patients. The furosemide stress test (FST) has been shown to predict the need for RRT and therefore could be used to exclude low-risk patients from enrollment in trials of RRT timing. We conducted this multicenter pilot study to determine whether FST could be used to screen patients at high risk for RRT and to determine the feasibility of incorporating FST into a trial of early initiation of RRT.
FST was performed using intravenous furosemide (1 mg/kg in furosemide-naive patients or 1.5 mg/kg in previous furosemide users). FST-nonresponsive patients (urine output less than 200 mL in 2 h) were then randomized to early (initiation within 6 h) or standard (initiation by urgent indication) RRT.
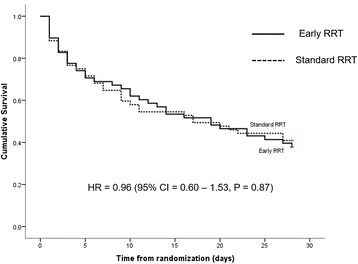
FST was completed in all patients (100%). Only 6/44 (13.6%) FST-responsive patients ultimately received RRT while 47/60 (78.3%) nonresponders randomized to standard RRT either received RRT or died (P < 0.001). Among 118 FST-nonresponsive patients, 98.3% in the early RRT arm and 75% in the standard RRT arm received RRT. The adherence to the protocol was 94.8% and 100% in the early and standard RRT group, respectively. We observed no differences in 28-day mortality (62.1 versus 58.3%, P = 0.68), 7-day fluid balance, or RRT dependence at day 28. However, hypophosphatemia occurred more frequently in the early RRT arm (P = 0.002).
The furosemide stress test appears to be feasible and effective in identifying patients for randomization to different RRT initiation times. Our findings should guide implementation of large-scale randomized controlled trials for the timing of RRT initiation.
clinicaltrials.gov, NCT02730117 . Registered 6 April 2016.
在严重急性肾损伤(AKI)中,开始肾脏替代治疗(RRT)的时机仍存在争议,早期开始治疗可能导致一些患者接受不必要的治疗,而期待治疗可能会延迟其他患者的 RRT。呋塞米应激试验(FST)已被证明可以预测 RRT 的需要,因此可以用于排除 RRT 时机试验中低风险患者的入组。我们进行了这项多中心试验,以确定 FST 是否可以用于筛选 RRT 风险高的患者,并确定将 FST 纳入早期 RRT 开始的试验中的可行性。
使用静脉注射呋塞米(呋塞米初治患者为 1mg/kg,之前使用过呋塞米的患者为 1.5mg/kg)进行 FST。FST 无反应的患者(2 小时内尿量少于 200mL)随后随机分为早期(6 小时内开始)或标准(根据紧急指征开始)RRT。
所有患者(100%)均完成了 FST。只有 6/44(13.6%)FST 反应患者最终接受了 RRT,而 47/60(78.3%)非反应者随机接受标准 RRT 治疗,或接受了 RRT 或死亡(P<0.001)。在 118 例 FST 无反应患者中,早期 RRT 组 98.3%和标准 RRT 组 75%接受了 RRT。早期和标准 RRT 组的方案依从性分别为 94.8%和 100%。我们观察到 28 天死亡率(62.1%比 58.3%,P=0.68)、7 天液体平衡或 28 天 RRT 依赖方面无差异。然而,早期 RRT 组更频繁发生低磷血症(P=0.002)。
呋塞米应激试验似乎可行且有效,可用于确定随机分组接受不同 RRT 开始时间的患者。我们的发现应该指导实施大规模的随机对照试验,以确定 RRT 开始的时机。
clinicaltrials.gov,NCT02730117。2016 年 4 月 6 日注册。