Ha Kyoung Hwa, Park Cheol Young, Jeong In Kyung, Kim Hyun Jin, Kim Sang Yong, Kim Won Jun, Yoon Ji Sung, Kim In Joo, Kim Dae Jung, Kim Sungrae
Department of Endocrinology and Metabolism, Ajou University School of Medicine, Suwon, Korea.
Cardiovascular and Metabolic Disease Etiology Research Center, Ajou University School of Medicine, Suwon, Korea.
Diabetes Metab J. 2018 Apr;42(2):137-146. doi: 10.4093/dmj.2018.42.2.137.
We evaluated the clinical characteristics of insulin resistance and β-cell dysfunction in newly diagnosed, drug-naive people with type 2 diabetes by analyzing nationwide cross-sectional data.
We collected the clinical data of 912 participants with newly diagnosed diabetes from 83 primary care clinics and hospitals nationwide from 2015 to 2016. The presence of insulin resistance and β-cell dysfunction was defined as a homeostatic model assessment of insulin resistance (HOMA-IR) value ≥2.5 and fasting C-peptide levels <1.70 ng/mL, respectively.
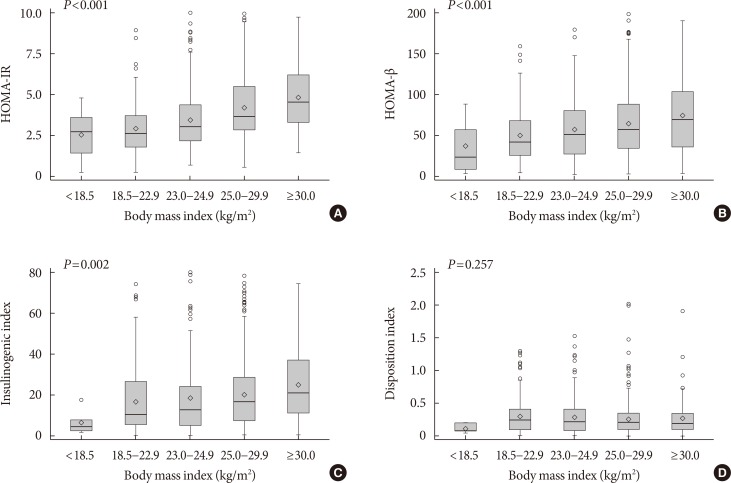
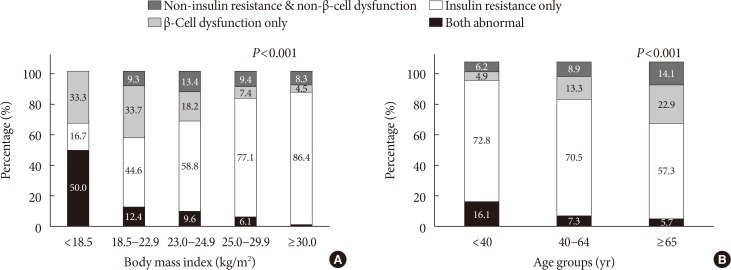
A total of 75.1% and 22.6% of participants had insulin resistance and β-cell dysfunction, respectively. The proportion of participants with insulin resistance but no β-cell dysfunction increased, and the proportion of participants with β-cell dysfunction but no insulin resistance decreased as body mass index (BMI) increased. People diagnosed with diabetes before 40 years of age had significantly higher HOMA-IR and BMI than those diagnosed over 65 years of age (HOMA-IR, 5.0 vs. 3.0; BMI, 28.7 kg/m² vs. 25.1 kg/m²). However, the β-cell function indices were lower in people diagnosed before 40 years of age than in those diagnosed after 65 years of age (homeostatic model assessment of β-cell function, 39.3 vs. 64.9; insulinogenic index, 10.3 vs. 18.7; disposition index, 0.15 vs. 0.25).
We observed that the main pathogenic mechanism of type 2 diabetes is insulin resistance in participants with newly diagnosed type 2 diabetes. In addition, young adults with diabetes are more likely to have higher insulin resistance with obesity and have higher insulin secretory defect with severe hyperglycemia in the early period of diabetes than older populations.
我们通过分析全国性横断面数据,评估了新诊断的、未接受过药物治疗的2型糖尿病患者胰岛素抵抗和β细胞功能障碍的临床特征。
我们收集了2015年至2016年全国83家基层医疗诊所和医院912例新诊断糖尿病患者的临床数据。胰岛素抵抗和β细胞功能障碍的存在分别定义为胰岛素抵抗稳态模型评估(HOMA-IR)值≥2.5和空腹C肽水平<1.70 ng/mL。
分别有75.1%和22.6%的参与者存在胰岛素抵抗和β细胞功能障碍。随着体重指数(BMI)增加,有胰岛素抵抗但无β细胞功能障碍的参与者比例上升,有β细胞功能障碍但无胰岛素抵抗的参与者比例下降。40岁之前被诊断为糖尿病的人群HOMA-IR和BMI显著高于65岁以上被诊断者(HOMA-IR,5.0对3.0;BMI,28.7kg/m²对25.1kg/m²)。然而,40岁之前被诊断的人群β细胞功能指标低于65岁之后被诊断的人群(β细胞功能稳态模型评估,39.3对64.9;胰岛素生成指数,10.3对18.7;处置指数,0.15对0.25)。
我们观察到,新诊断的2型糖尿病患者中2型糖尿病的主要致病机制是胰岛素抵抗。此外,与老年人群相比,糖尿病青年成年人在糖尿病早期更易因肥胖出现更高的胰岛素抵抗,且因严重高血糖出现更高的胰岛素分泌缺陷。