Ren W, Gao L, Li S, Chen C, Li F, Wang Q, Zhi Y, Song J, Dou Z, Xue L, Zhi K
Department of Oral and Maxillofacial Surgery, The affiliated hospital of Qingdao University, No.1677, Wutai mountain Road, Qingdao, Shandong, P. R. China. 255666
Med Oral Patol Oral Cir Bucal. 2018 May 1;23(3):e359-e366. doi: 10.4317/medoral.22295.
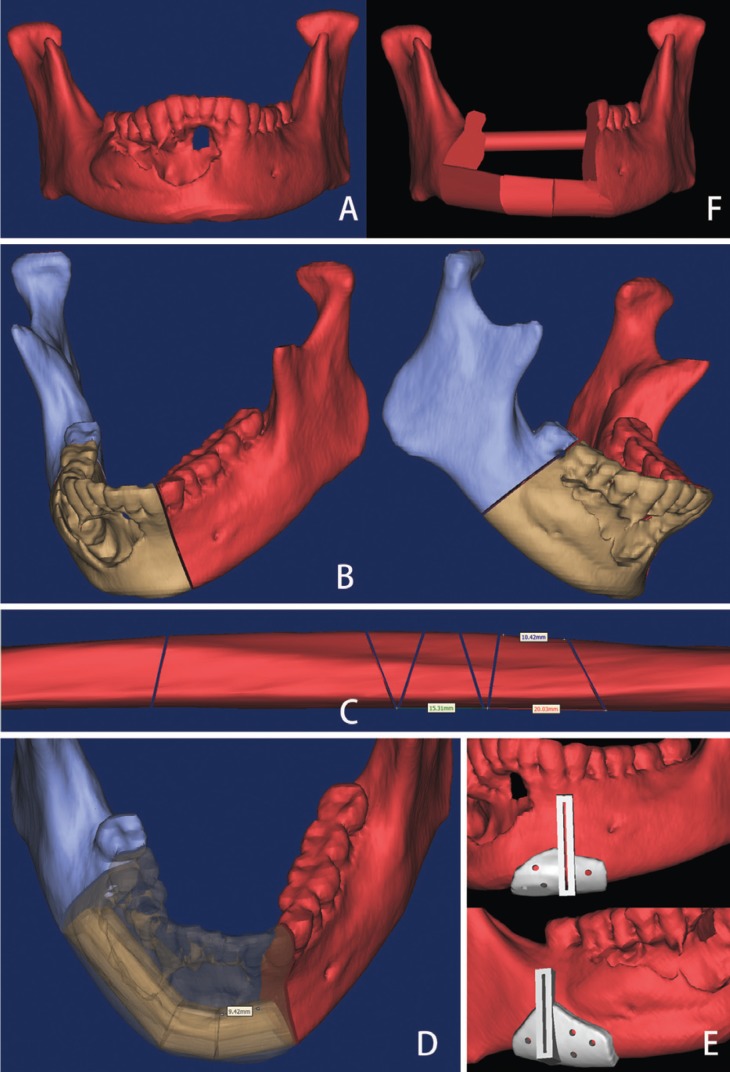
This study was to evaluate the use of virtual planning and 3D printing modeling in mandibular reconstruction and compare the operation time and surgical outcome of this technique with conventional method.
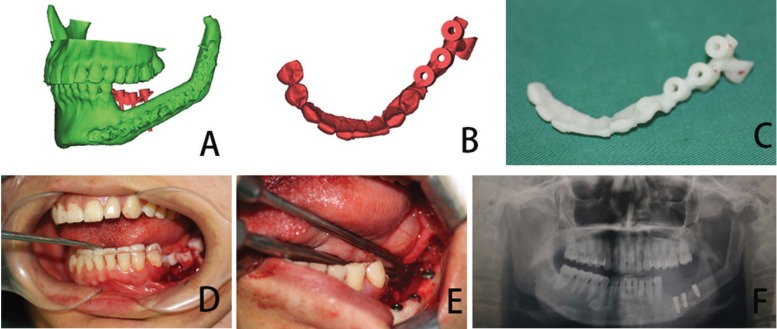
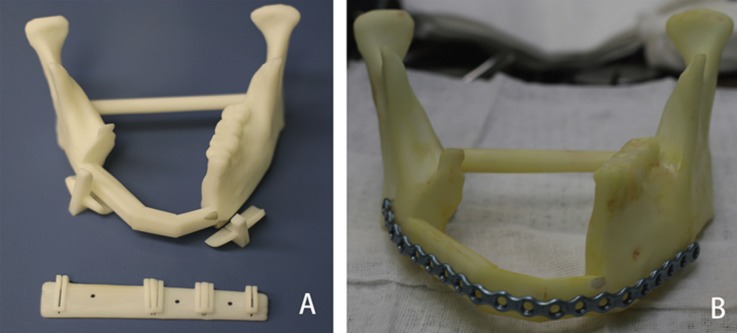
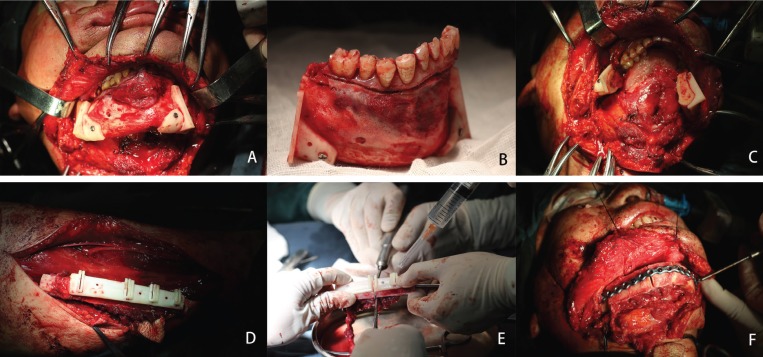
Between 2014 and 2017, 15 patients underwent vascularized fibula flap mandibular reconstruction using virtual planning and 3D printing modeling. Titanium plates were pre-bent using the models and cutting guides were used for osteotomies. 15 patients who underwent mandibular reconstruction using fibula flap without aid of virtual planning and 3D printing models were selected as control group. The operation time was recorded and compared in two groups. Accuracy of reconstruction was measured by superimposing the preoperative image onto the postoperative image of mandible. The selected bony landmark, distance and angle were measured.
The mean total operation time and reconstruction time were 1.60±0.37 and 5.54±0.50 hours in computer-assisted group, respectively; These were 2.58±0.45 and 6.54±0.70 hours in conventional group, respectively. Both operation time and reconstruction time were shorter in computer-assisted group. The difference between the preoperative and postoperative intercondylar distances, intergonial angle distances, anteroposterior distances and gonial angles were 2.92±1.15 and 4.48±1.41mm, 2.93±1.19 and 4.79±1.48mm, 4.31±1.24 and 5.61±1.41mm, 3.85±1.68° and 5.88±2.12° in the computer-assisted and conventional group, respectively. The differences between the preoperative and postoperative mandible is smaller in the computer-assisted group.
Virtual planning and 3D printing modeling have the potential to increase mandibular reconstruction accuracy and reduce operation time. we believe that this technology for mandibular reconstruction in selected patients will become a used method and improve the quality of reconstruction.
本研究旨在评估虚拟规划和3D打印建模在下颌骨重建中的应用,并将该技术的手术时间和手术效果与传统方法进行比较。
2014年至2017年期间,15例患者采用虚拟规划和3D打印建模进行血管化腓骨瓣下颌骨重建。使用模型对钛板进行预弯,并使用切割导板进行截骨术。选择15例未借助虚拟规划和3D打印模型而采用腓骨瓣进行下颌骨重建的患者作为对照组。记录并比较两组的手术时间。通过将术前图像与下颌骨术后图像叠加来测量重建的准确性。测量选定的骨标志、距离和角度。
计算机辅助组的平均总手术时间和重建时间分别为1.60±0.37小时和5.54±0.50小时;传统组分别为2.58±0.45小时和6.54±0.70小时。计算机辅助组的手术时间和重建时间均较短。计算机辅助组和传统组术前与术后髁间距离、下颌角间角度距离、前后距离和下颌角的差异分别为2.92±1.15和4.48±1.41mm、2.93±1.19和4.79±1.48mm、4.31±1.24和5.61±1.41mm、3.85±1.68°和5.88±2.12°。计算机辅助组术前与术后下颌骨的差异较小。
虚拟规划和3D打印建模有可能提高下颌骨重建的准确性并减少手术时间。我们相信,这种用于特定患者下颌骨重建的技术将成为一种常用方法并提高重建质量。