Xu Jia, Rosen Milan, Luffman Christina I, Law Charles, Laloo Anita, Rosen Seymour, Faulkner-Jones Beverly E
Department of Pathology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts, USA.
Kitware Inc., Clifton Park, New York, USA.
Case Rep Nephrol Dial. 2018 Mar 2;8(1):35-44. doi: 10.1159/000487262. eCollection 2018 Jan-Apr.
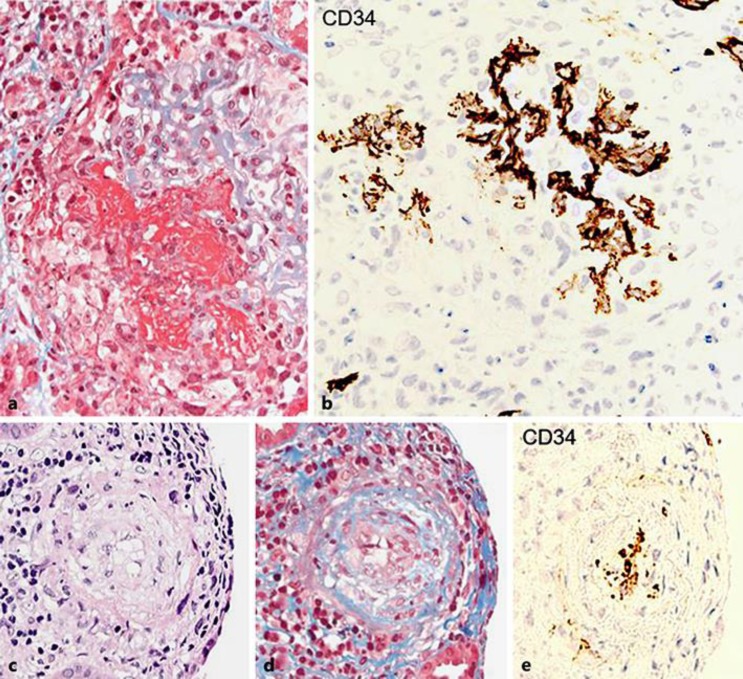
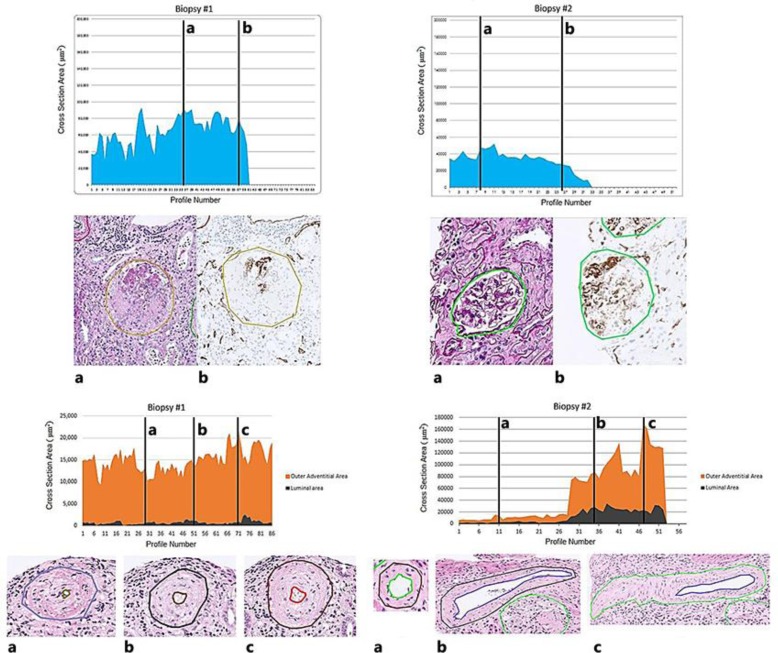
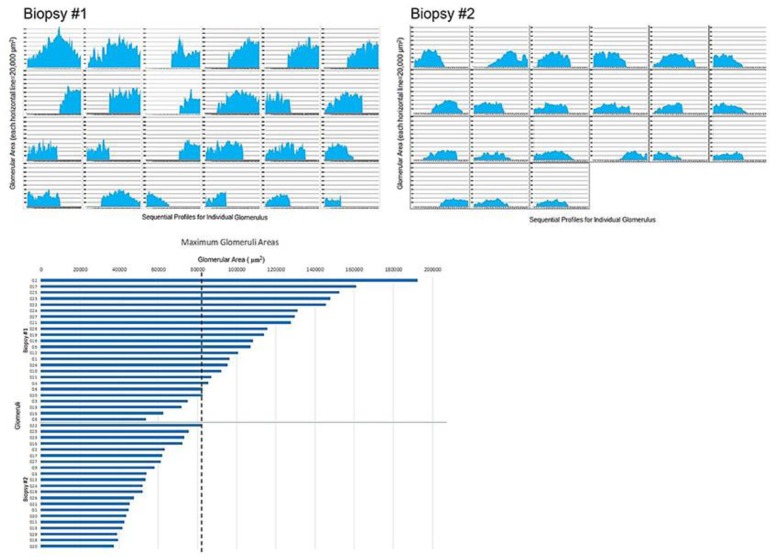
Scleroderma vasculopathy and ANCA (antineutrophil cytoplasmic antibodies)-associated glomerulonephritis have rarely been reported to occur simultaneously in one patient. Herein, we report a patient who presented with a classic constellation of clinical and laboratory findings of systemic scleroderma and was subsequently found to be positive for p-ANCA. Two renal biopsies, performed 5 months apart, demonstrated typical changes of the two entities in both acute and "healed" phases, which were analyzed by computer mapping techniques. The two renal biopsies were serially sectioned and stained routinely, and with CD31 and CD34 as endothelial markers. The slides were digitized, aligned and analyzed. Each glomerular tuft was sequentially studied in terms of total area (µm) and each biopsy was individually profiled. All arterial vessels were sequentially studied with whole vessel and luminal areas delineated and ratios calculated. The initial biopsy contained 32 glomeruli almost all with extensive fibrinoid necrosis and destruction of the capillary network. The arterial vessels (interlobular and arcuate) showed intimal edema with luminal occlusion. CD31/CD34 stains showed variable endothelial intactness but demonstrated the luminal size shifts. The second biopsy had 37 glomeruli that were either segmentally or globally sclerotic with no active changes. The vessels were now normally patent. Each glomerular tuft and arterial vessel in both biopsies was analyzed as a serial section histogram documenting these changes. These studies depict the rare occurrence of two entities together, the scleroderma kidney vasculopathy and the glomerulonephritis of ANCA-associated vasculitis syndrome both in an acute and healing phase, profiled by computer mapping techniques.
硬皮病血管病变与抗中性粒细胞胞浆抗体(ANCA)相关的肾小球肾炎很少有报道在同一患者中同时发生。在此,我们报告一名患者,其表现出系统性硬皮病的典型临床和实验室检查结果,随后被发现p-ANCA呈阳性。在相隔5个月进行的两次肾活检中,均显示出这两种疾病在急性和“愈合”阶段的典型变化,并通过计算机绘图技术进行了分析。两次肾活检标本均进行连续切片并常规染色,同时用CD31和CD34作为内皮标志物进行染色。将玻片数字化、对齐并分析。对每个肾小球丛依次研究其总面积(μm),并对每次活检进行单独分析。对所有动脉血管依次进行研究,勾勒出整个血管和管腔面积并计算比值。初次活检包含32个肾小球,几乎所有肾小球都有广泛的纤维蛋白样坏死和毛细血管网破坏。动脉血管(小叶间动脉和弓状动脉)显示内膜水肿伴管腔闭塞。CD31/CD34染色显示内皮完整性各异,但显示了管腔大小的变化。第二次活检有37个肾小球,呈节段性或全球性硬化,无活动性改变。血管现已正常通畅。对两次活检中的每个肾小球丛和动脉血管进行分析,作为记录这些变化的连续切片直方图。这些研究描绘了硬皮病肾血管病变和ANCA相关血管炎综合征的肾小球肾炎这两种疾病在急性和愈合阶段同时罕见发生的情况,并通过计算机绘图技术进行了分析。