Muthukrishnan Meera, Sutcliffe Siobhan, Hunleth Jean M, Wang Jean S, Colditz Graham A, James Aimee S
Department of Epidemiology and Biostatistics, Saint Louis University College of Public Health and Social Justice, St. Louis, MO, USA.
Division of Public Health Sciences, Department of Surgery, Washington University School of Medicine, St. Louis, MO, USA.
Contemp Clin Trials Commun. 2018 Mar 6;10:29-35. doi: 10.1016/j.conctc.2018.02.005. eCollection 2018 Jun.
Colorectal cancer (CRC) is the second most common cancer in the US. Despite evidence that screening reduces CRC incidence and mortality, screening rates are sub-optimal with disparities by race/ethnicity, income, and geography. Rural-urban differences in CRC screening are understudied even though approximately one-fifth of the US population lives in rural areas. This focus on urban populations limits the generalizability and dissemination potential of screening interventions.
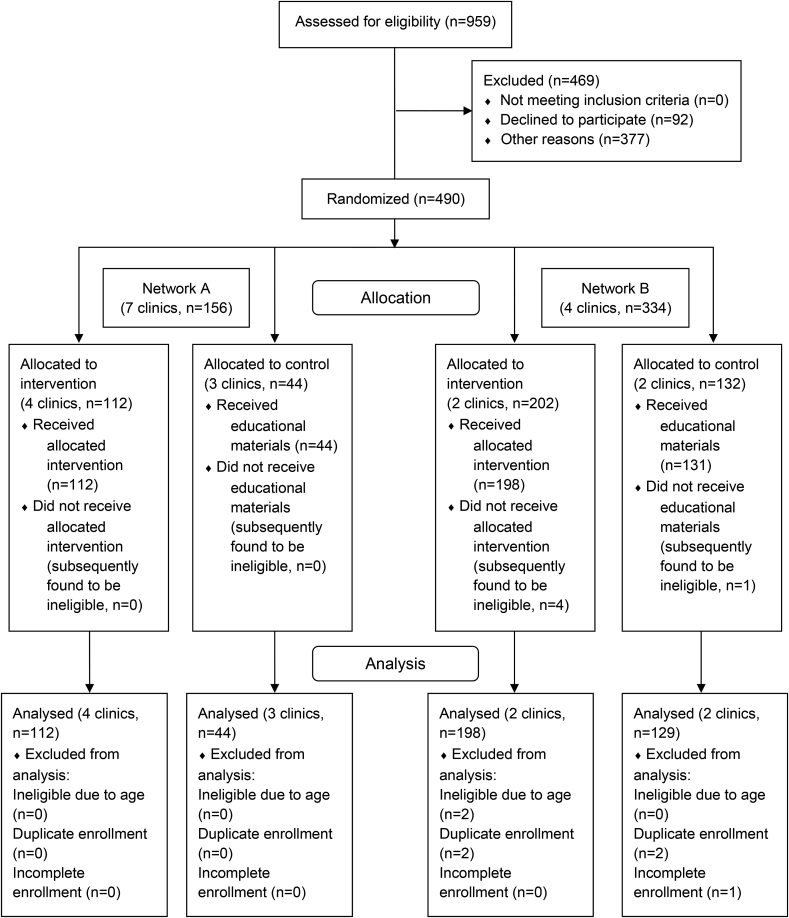
Using community-based participatory research (CBPR) principles, we designed a cluster-randomized trial, adaptable to a range of settings, including rural and urban health centers. We enrolled 483 participants across 11 health centers representing 2 separate networks. Both networks serve medically-underserved communities; however one is primarily rural and one primarily urban.
Our goal in this analysis is to describe baseline characteristics of participants and examine setting-level differences. CBPR was a critical for recruiting networks to the trial. Patient respondents were predominately female (61.3%), African-American (66.5%), and earned <$1200 per month (87.1%). The rural network sample was older; more likely to be female, white, disabled or retired, and have a higher income, but fewer years of education.
Variation in the samples partly reflects the CBPR process and partly reflects inherent differences in the communities. This confirmed the importance of using CBPR when planning for eventual dissemination, as it enhanced our ability to work within diverse settings. These baseline findings indicate that using a uniform approach to implementing a trial or intervention across diverse settings might not be effective or efficient.
结直肠癌(CRC)是美国第二大常见癌症。尽管有证据表明筛查可降低结直肠癌的发病率和死亡率,但筛查率仍未达到最佳水平,且在种族/族裔、收入和地理位置方面存在差异。尽管美国约五分之一的人口生活在农村地区,但对结直肠癌筛查的城乡差异研究不足。对城市人口的关注限制了筛查干预措施的普遍性和推广潜力。
我们运用基于社区的参与性研究(CBPR)原则,设计了一项整群随机试验,该试验适用于包括农村和城市健康中心在内的一系列环境。我们在代表两个独立网络的11个健康中心招募了483名参与者。两个网络都为医疗服务不足的社区提供服务;然而,一个主要是农村社区,另一个主要是城市社区。
我们本次分析的目的是描述参与者的基线特征,并检查不同环境水平的差异。CBPR对于招募各网络参与试验至关重要。患者受访者主要为女性(61.3%)、非裔美国人(66.5%),且月收入低于1200美元(87.1%)。农村网络样本年龄更大;更有可能是女性、白人、残疾或退休人员,且收入较高,但受教育年限较少。
样本的差异部分反映了CBPR过程,部分反映了社区的固有差异。这证实了在规划最终推广时使用CBPR的重要性,因为它增强了我们在不同环境中开展工作的能力。这些基线研究结果表明,在不同环境中采用统一方法实施试验或干预可能无效或低效。