Steno Diabetes Center Copenhagen, Copenhagen, Denmark.
Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark.
PLoS One. 2018 Apr 26;13(4):e0196634. doi: 10.1371/journal.pone.0196634. eCollection 2018.
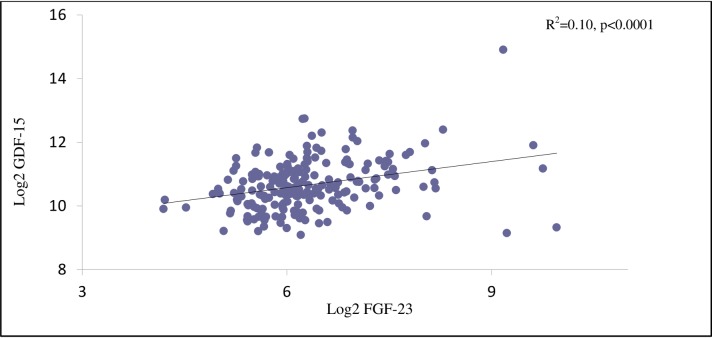
Two biomarkers, growth differentiation factor 15 (GDF-15) and fibroblast growth factor 23 (FGF-23)), reflecting different aspects of renal pathophysiology, were evaluated as determinants of decline in estimated glomerular filtration rate (eGFR), incident cardiovascular disease (CVD) and all-cause mortality in patients with type 2 diabetes (T2D) and microalbuminuria, but without clinical cardiac disease.
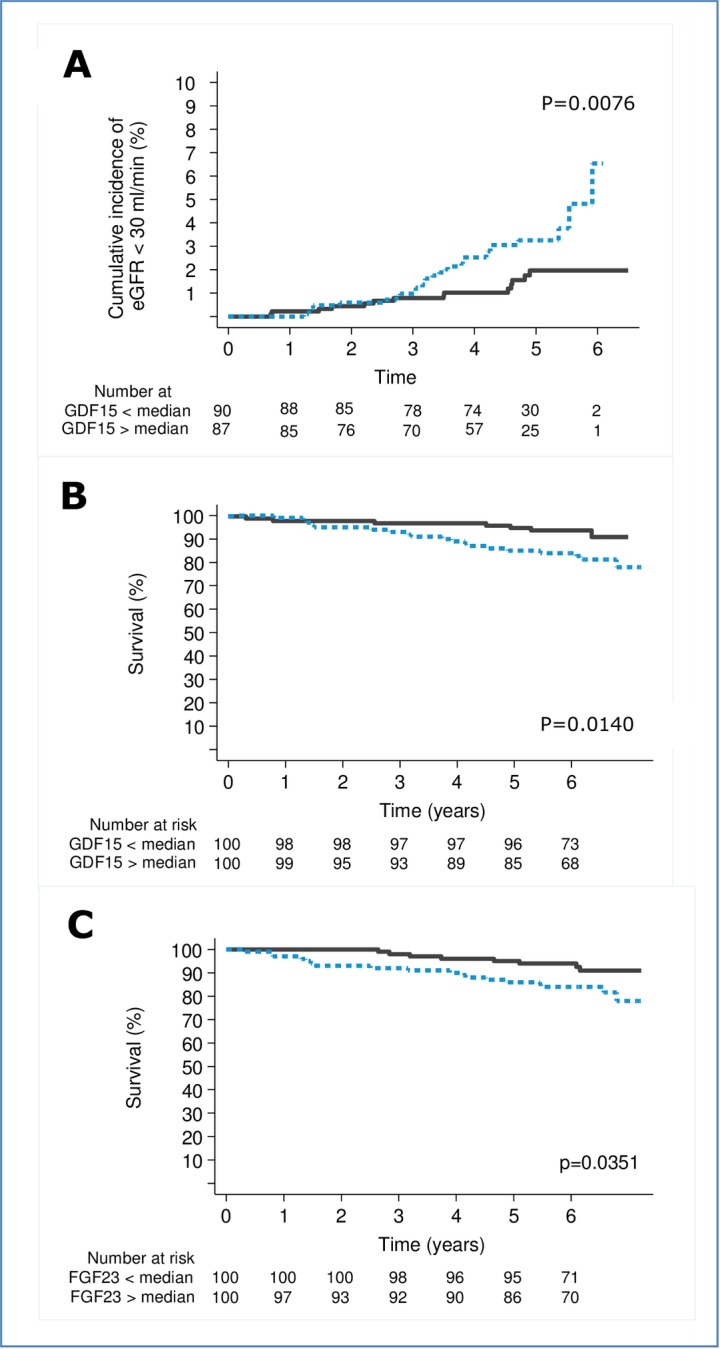
Prospective study including 200 T2D patients. The predefined endpoint of chronic kidney disease (CKD) progression: A decline in eGFR of >30% at any time point during follow-up. Hazard ratios (HR) are provided per 1 SD increment of log2-transformed values.
Mean (± SD) age was 59 ± 9 years, eGFR 91.1 ± 18.3 ml/min/1.73m2 and median (IQR) UAER 103 (39-230) mg/24-h. During a median 6.1 years follow-up, 40 incident CVD events, 26 deaths and 42 patients reached the CKD endpoint after median 4.9 years. Higher GDF-15 was a determinant of decline in eGFR >30% and all-cause mortality in adjusted models (HR 1.7 (1.1-2.5); p = 0.018 and HR 1.9 (1.2-2.9); p = 0.003, respectively). Adding GDF-15 to traditional risk factors improved risk prediction of decline in renal function (relative integrated discrimination improvement (rIDI) = 30%; p = 0.037). Higher FGF-23 was associated with all-cause mortality in adjusted models (HR 1.6 (1.1-2.2); p = 0.011) with a rIDI of 30% (p = 0.024).
In patients with T2D and microalbuminuria, higher GDF-15 and FGF-23 were independently associated with all-cause mortality and higher GDF-15 improved risk prediction of decline in kidney function and higher FGF-23 of all-cause mortality, beyond traditional risk factors, but not independently of GDF-15.
生长分化因子 15(GDF-15)和成纤维细胞生长因子 23(FGF-23)这两种生物标志物反映了肾脏病理生理学的不同方面,它们被评估为 2 型糖尿病(T2D)和微量白蛋白尿患者肾小球滤过率(eGFR)下降、心血管疾病(CVD)事件和全因死亡率的决定因素,但这些患者没有临床心脏疾病。
前瞻性研究包括 200 名 T2D 患者。慢性肾脏病(CKD)进展的预设终点:在随访期间的任何时间点 eGFR 下降>30%。每增加 1 SD 对数转换值的危险比(HR)。
平均(± SD)年龄为 59 ± 9 岁,eGFR 为 91.1 ± 18.3 ml/min/1.73m2,中位(IQR)UAER 为 103(39-230)mg/24-h。在中位 6.1 年的随访期间,40 例发生 CVD 事件,26 例死亡,42 例患者在中位 4.9 年后达到 CKD 终点。调整模型中,较高的 GDF-15 是 eGFR>30%和全因死亡率下降的决定因素(HR 1.7(1.1-2.5);p = 0.018 和 HR 1.9(1.2-2.9);p = 0.003)。将 GDF-15 添加到传统危险因素中可改善肾功能下降的风险预测(相对综合判别改善(rIDI)=30%;p = 0.037)。较高的 FGF-23 与调整模型中的全因死亡率相关(HR 1.6(1.1-2.2);p = 0.011),rIDI 为 30%(p = 0.024)。
在患有 T2D 和微量白蛋白尿的患者中,较高的 GDF-15 和 FGF-23 与全因死亡率独立相关,较高的 GDF-15 改善了肾功能下降的风险预测,而较高的 FGF-23 则与全因死亡率相关,超过了传统危险因素,但与 GDF-15 无关。