Steno Diabetes Center Copenhagen, Niels Steensens Vej 2, 2820, Gentofte, Denmark.
Department of Clinical Chemistry, VU University Medical Center, Amsterdam, The Netherlands.
Cardiovasc Diabetol. 2017 Jul 11;16(1):88. doi: 10.1186/s12933-017-0569-8.
To evaluate symmetric dimethylarginine (SDMA) and asymmetric dimethylarginine (ADMA) as risk markers of cardiovascular disease, all-cause mortality and deterioration in renal function in a well characterised type 2 diabetic population with microalbuminuria and without symptoms of coronary artery disease.
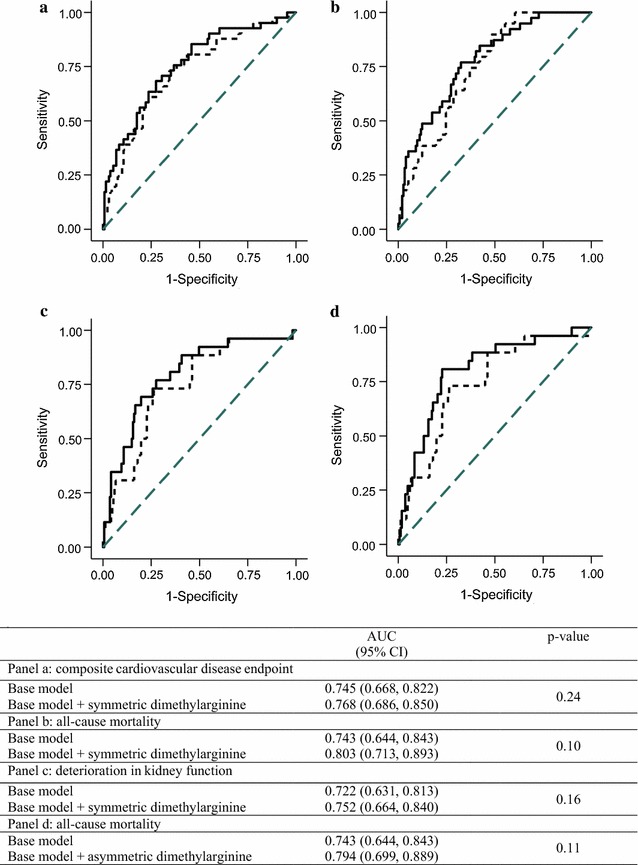
200 participants followed for 6.1 years. SDMA and ADMA were measured at baseline. Endpoints included (1) composite cardiovascular endpoint (n = 40); (2) all-cause mortality (n = 26); and (3) decline in eGFR of >30% (n = 42). Cox models were unadjusted and adjusted for traditional risk factors (sex, age, systolic blood pressure, LDL-cholesterol, smoking, HbA, creatinine and urinary albumin excretion rate). To assess if SDMA or ADMA improved risk prediction beyond traditional risk factors we calculated c statistics and relative integrated discrimination improvement (rIDI). C statistic (area under the curve) quantifies the model's improved ability to discriminate events from non-events. rIDI quantifies the increase in separation of events and non-events on a relative scale.
Higher SDMA was associated with increased risk of all three endpoints (unadjusted: p ≤ 0.001; adjusted: p ≤ 0.02). Higher ADMA was associated with all-cause mortality (unadjusted: p = 0.002; adjusted: p = 0.006), but not cardiovascular disease or decline in eGFR (p ≥ 0.29).The c statistic was not significant for any of the endpoints for either SDMA or ADMA (p ≥ 0.10). The rIDI for SDMA was 15.0% (p = 0.081) for the cardiovascular endpoint, 52.5% (p = 0.025) for all-cause mortality and 48.8% (p = 0.007) for decline in eGFR; for ADMA the rIDI was 49.1% (p = 0.017) for all-cause mortality.
In persons with type 2 diabetes and microalbuminuria higher SDMA was associated with incident cardiovascular disease, all-cause mortality and deterioration in renal function. Higher ADMA was associated with all-cause mortality. SDMA and ADMA significantly improved risk prediction for all-cause mortality, and SDMA for deterioration in renal function beyond traditional risk factors.
为了评估对称二甲基精氨酸(SDMA)和非对称二甲基精氨酸(ADMA)作为心血管疾病、全因死亡率和肾功能恶化的风险标志物,我们在患有微量白蛋白尿且无冠心病症状的 2 型糖尿病患者中进行了一项特征明确的研究。
200 名参与者随访 6.1 年。在基线时测量了 SDMA 和 ADMA。终点包括(1)复合心血管终点(n=40);(2)全因死亡率(n=26);(3)eGFR 下降>30%(n=42)。Cox 模型未调整,调整了传统危险因素(性别、年龄、收缩压、LDL-胆固醇、吸烟、HbA、肌酐和尿白蛋白排泄率)。为了评估 SDMA 或 ADMA 是否能改善传统危险因素以外的风险预测,我们计算了 C 统计量和相对综合判别改善(rIDI)。C 统计量(曲线下面积)量化了模型对事件和非事件的区分能力的提高。rIDI 量化了事件和非事件在相对尺度上的分离程度的增加。
较高的 SDMA 与所有三个终点的风险增加相关(未调整:p≤0.001;调整:p≤0.02)。较高的 ADMA 与全因死亡率相关(未调整:p=0.002;调整:p=0.006),但与心血管疾病或 eGFR 下降无关(p≥0.29)。SDMA 或 ADMA 对任何终点的 C 统计量均无统计学意义(p≥0.10)。SDMA 的 rIDI 为心血管终点的 15.0%(p=0.081),全因死亡率的 52.5%(p=0.025),eGFR 下降的 48.8%(p=0.007);ADMA 的 rIDI 为全因死亡率的 49.1%(p=0.017)。
在 2 型糖尿病合并微量白蛋白尿的患者中,较高的 SDMA 与心血管疾病、全因死亡率和肾功能恶化的发生有关。较高的 ADMA 与全因死亡率有关。SDMA 和 ADMA 显著改善了全因死亡率的风险预测,SDMA 改善了肾功能恶化的风险预测,优于传统危险因素。