Pereira Hélder, Caldeira Daniel, Teles Rui Campante, Costa Marco, da Silva Pedro Canas, da Gama Ribeiro Vasco, Brandão Vítor, Martins Dinis, Matias Fernando, Pereira-Machado Francisco, Baptista José, Abreu Pedro Farto E, Santos Ricardo, Drummond António, de Carvalho Henrique Cyrne, Calisto João, Silva João Carlos, Pipa João Luís, Marques Jorge, Sousa Paulino, Fernandes Renato, Ferreira Rui Cruz, Ramos Sousa, Oliveira Eduardo Infante, de Sousa Almeida Manuel
Serviço de Cardiologia, Hospital Garcia de Orta EPE, Avenida Prof. Torrado da Silva, 2801-951, Almada, Portugal.
Centro Cardiovascular da Universidade de Lisboa (CCUL), CAML, Faculdade de Medicina, Universidade de Lisboa, Avenida Professor Egas Moniz, Lisboa, 1649-028, Portugal.
BMC Cardiovasc Disord. 2018 Apr 24;18(1):69. doi: 10.1186/s12872-018-0794-4.
We aimed to evaluate the impact of thrombus aspiration (TA) during primary percutaneous coronary intervention (P-PCI) in 'real-world' settings.
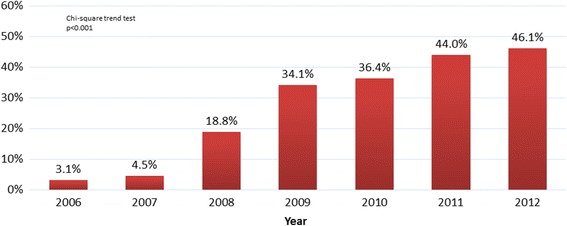
We performed a retrospective study, using data from the National Registry of Interventional Cardiology (RNCI 2006-2012, Portugal) with ST-elevation myocardial infarction (STEMI) patients treated with P-PCI. The primary outcome, in-hospital mortality, was analysed through adjusted odds ratio (aOR) and 95% confidence intervals (95%CI).
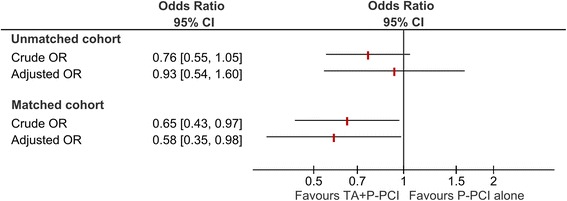
We assessed data for 9458 STEMI patients that undergone P-PCI (35% treated with TA). The risk of in-hospital mortality with TA (aOR 0.93, 95%CI:0.54-1.60) was not significantly decreased. After matching patients through the propensity score, TA reduced significantly the risk of in-hospital mortality (OR 0.58, 95%CI:0.35-0.98; 3500 patients).
The whole cohort data does not support the routine use of TA in P-PCI, but the results of the propensity-score matched cohort suggests that the use of selective TA may improve the short-term risks of STEMI.
我们旨在评估在“真实世界”环境下,在直接经皮冠状动脉介入治疗(P-PCI)期间进行血栓抽吸(TA)的影响。
我们进行了一项回顾性研究,使用来自葡萄牙国家介入心脏病学注册中心(RNCI 2006 - 2012)中接受P-PCI治疗的ST段抬高型心肌梗死(STEMI)患者的数据。通过调整后的优势比(aOR)和95%置信区间(95%CI)分析主要结局,即住院死亡率。
我们评估了9458例接受P-PCI的STEMI患者的数据(35%接受TA治疗)。TA治疗组的住院死亡风险(aOR 0.93,95%CI:0.54 - 1.60)没有显著降低。通过倾向评分匹配患者后,TA显著降低了住院死亡风险(OR 0.58,95%CI:0.35 - 0.98;3500例患者)。
整个队列数据不支持在P-PCI中常规使用TA,但倾向评分匹配队列的结果表明,选择性使用TA可能会改善STEMI的短期风险。