Department of Epidemiology, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
Department of Intensive Care Medicine, University Medical Center Utrecht, Utrecht University, Room F06.149, P.O. Box 85500, 3508 GA, Utrecht, The Netherlands.
Eur J Clin Microbiol Infect Dis. 2018 Jul;37(7):1333-1344. doi: 10.1007/s10096-018-3255-1. Epub 2018 Apr 26.
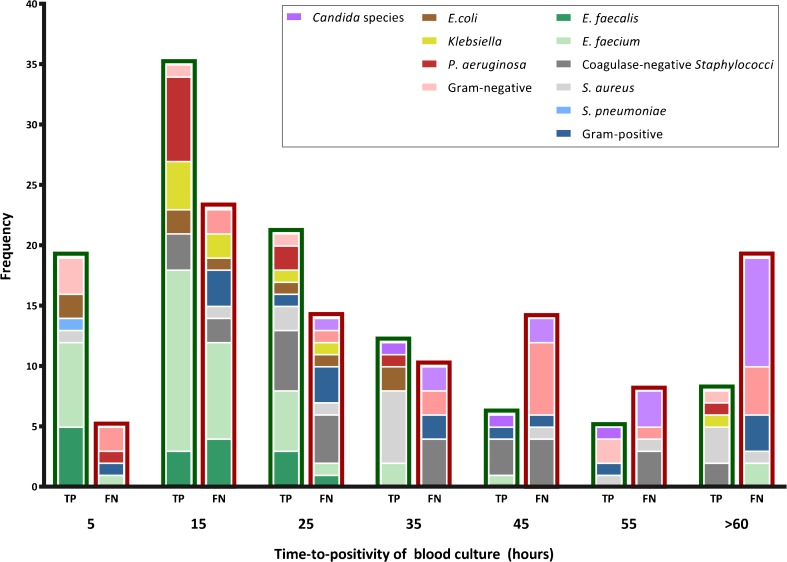
Molecular tests may enable early adjustment of antimicrobial therapy and be complementary to blood culture (BC) which has imperfect sensitivity in critically ill patients. We evaluated a novel multiplex real-time PCR assay to diagnose bloodstream pathogens directly in whole blood samples (BSI-PCR). BSI-PCR included 11 species- and four genus-specific PCRs, a molecular Gram-stain PCR, and two antibiotic resistance markers. We collected 5 mL blood from critically ill patients simultaneously with clinically indicated BC. Microbial DNA was isolated using the Polaris method followed by automated DNA extraction. Sensitivity and specificity were calculated using BC as reference. BSI-PCR was evaluated in 347 BC-positive samples (representing up to 50 instances of each pathogen covered by the test) and 200 BC-negative samples. Bacterial species-specific PCR sensitivities ranged from 65 to 100%. Sensitivity was 26% for the Gram-positive PCR, 32% for the Gram-negative PCR, and ranged 0 to 7% for yeast PCRs. Yeast detection was improved to 40% in a smaller set-up. There was no overall association between BSI-PCR sensitivity and time-to-positivity of BC (which was highly variable), yet Ct-values were lower for true-positive versus false-positive PCR results. False-positive results were observed in 84 (4%) of the 2200 species-specific PCRs in 200 culture-negative samples, and ranged from 0 to 6% for generic PCRs. Sensitivity of BSI-PCR was promising for individual bacterial pathogens, but still insufficient for yeasts and generic PCRs. Further development of BSI-PCR will focus on improving sensitivity by increasing input volumes and on subsequent implementation as a bedside test.
分子检测可实现抗菌治疗的早期调整,并与血培养(BC)互补,后者在重症患者中敏感性不高。我们评估了一种新型多重实时 PCR 检测方法,以直接从全血样本中诊断血流感染病原体(BSI-PCR)。BSI-PCR 包括 11 种种属特异性和 4 种属特异性 PCR、分子革兰氏染色 PCR 和 2 种抗生素耐药性标记物。我们同时从重症患者采集 5mL 血液,同时进行临床指示的 BC。使用 Polaris 方法分离微生物 DNA,然后进行自动 DNA 提取。以 BC 为参考计算灵敏度和特异性。BSI-PCR 在 347 份 BC 阳性样本(代表该检测涵盖的每种病原体最多 50 个实例)和 200 份 BC 阴性样本中进行了评估。细菌种属特异性 PCR 灵敏度为 65%至 100%。革兰氏阳性 PCR 的灵敏度为 26%,革兰氏阴性 PCR 的灵敏度为 32%,酵母 PCR 的灵敏度为 0 至 7%。在较小的设置中,酵母检测的灵敏度提高到 40%。BSI-PCR 的灵敏度与 BC 的阳性时间(高度可变)之间没有总体关联,但 Ct 值对于真阳性与假阳性 PCR 结果较低。在 200 份无培养物的样本中,2200 份种属特异性 PCR 中有 84 份(4%)出现假阳性结果,通用 PCR 的假阳性率为 0 至 6%。BSI-PCR 对个别细菌病原体的灵敏度很有前景,但对酵母和通用 PCR 仍然不足。BSI-PCR 的进一步开发将侧重于通过增加输入量来提高灵敏度,并随后作为床边检测进行实施。