Infectious Disease Epidemiology Group, Weill Cornell Medicine-Qatar, Cornell University, Qatar Foundation - Education City, Doha, Qatar.
Population Health Research Institute, St George's, University of London, London, United Kingdom.
PLoS One. 2018 Apr 30;13(4):e0196613. doi: 10.1371/journal.pone.0196613. eCollection 2018.
Objective was to examine the temporal variation of HIV sero-discordancy in select representative countries (Kenya, Lesotho, Mali, Niger, Tanzania, and Zimbabwe) in sub-Saharan Africa at different HIV epidemic scales. A sero-discordant couple is defined as a stable couple (SC) in which one partner is HIV-positive while the other is HIV-negative.
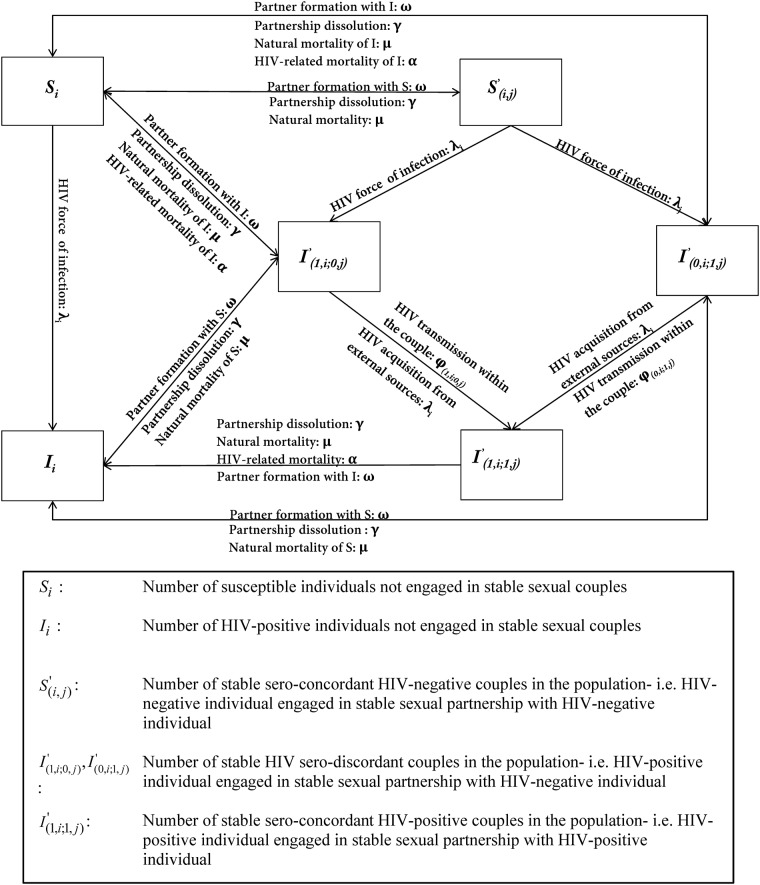
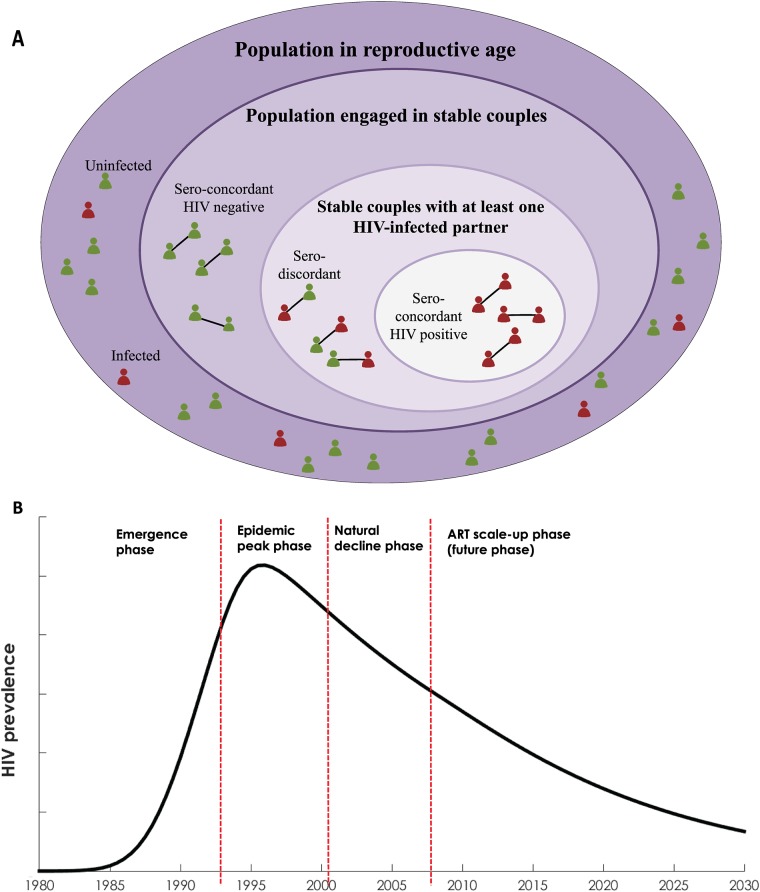
A deterministic compartmental mathematical model was constructed to describe HIV transmission dynamics. The model was pair-based, that is explicitly modeling formation of SCs and infection dynamics in both SCs and in single individuals. The model accommodated for different forms of infection statuses in SCs. Using population-based nationally-representative epidemiologic and demographic input data, historical (1980-2014) and future (2015-2030) trends of sero-discordancy and other demographic and epidemiologic indicators were projected throughout HIV epidemic phases.
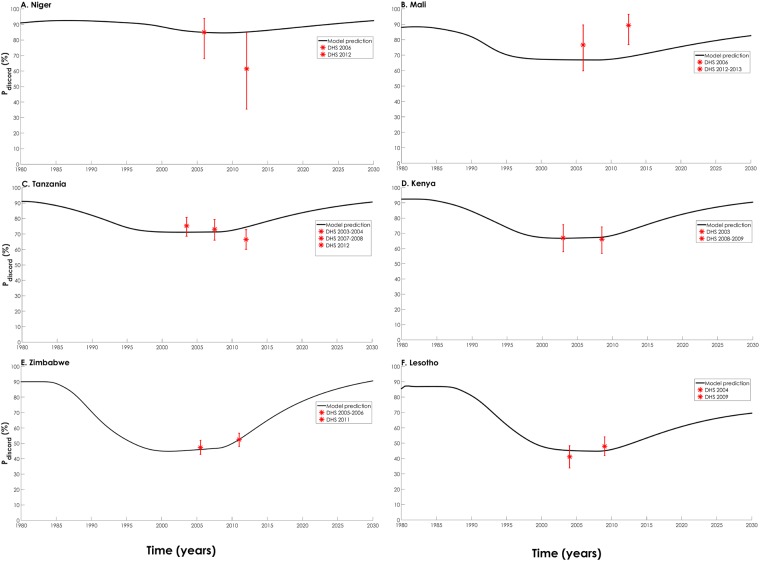
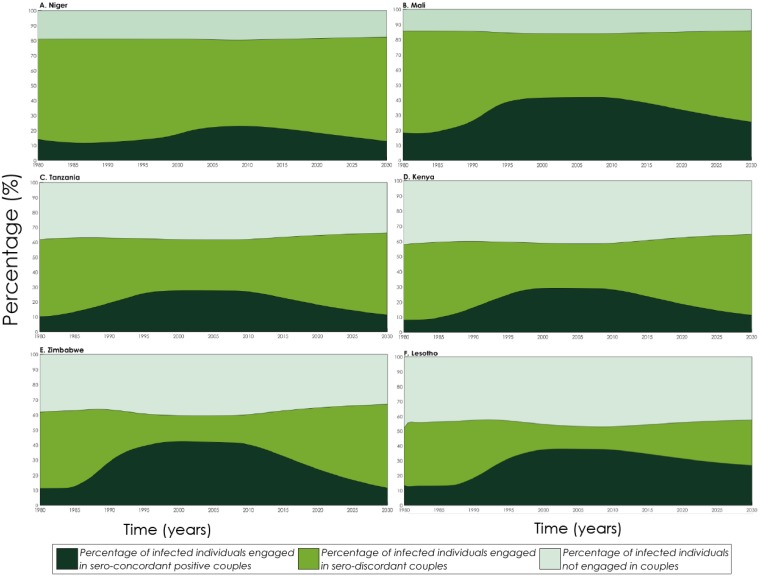
As the epidemics emerged, about 90% of SCs affected by HIV were sero-discordant. This proportion declined to 45%-88% at epidemic peak and stabilized as the epidemics started their natural decline. The largest reductions in sero-discordancy were in high HIV-prevalence countries. As the epidemics further declined with antiretroviral therapy (ART) scale-up, the proportion of sero-discordant couples among HIV-affected couples was projected to increase to 70%-92% by 2030. The proportion of sero-discordant couples among all SCs increased as the epidemics emerged and evolved, then peaked at 2%-20% as the epidemics peaked, and then declined as the epidemics declined to reach 0.3%-16% by 2030.
Sero-discordancy patterns varied with the evolution of the epidemics, and were affected by both epidemic phase and scale. The largest variations were found in high HIV-prevalence countries. The fraction of stable couples that are sero-discordant, as opposed to being sero-concordant positive, was projected to increase with ART scale-up and further HIV incidence decline over the coming two decades. These findings inform strategic planning and resource allocation for interventions among sero-discordant couples.
本研究旨在探讨在不同艾滋病毒流行规模的撒哈拉以南非洲选定代表性国家(肯尼亚、莱索托、马里、尼日尔、坦桑尼亚和津巴布韦)中,艾滋病毒血清不一致的时间变化。血清不一致的夫妇是指一方为艾滋病毒阳性而另一方为艾滋病毒阴性的稳定夫妇。
我们构建了一个确定性的房室数学模型来描述艾滋病毒传播动力学。该模型基于对,即明确建模稳定夫妇的形成以及稳定夫妇和单身个体中的感染动态。该模型适应了稳定夫妇中不同形式的感染状况。利用基于人群的全国代表性流行病学和人口统计学输入数据,对 1980 年至 2014 年的历史(1980-2014 年)和未来(2015-2030 年)血清不一致以及其他人口统计学和流行病学指标的趋势进行了预测,贯穿整个艾滋病毒流行阶段。
随着疫情的出现,约 90%的受艾滋病毒影响的稳定夫妇血清不一致。这一比例在流行高峰期下降到 45%-88%,随着疫情开始自然下降而稳定下来。血清不一致的最大减少发生在艾滋病毒高流行国家。随着抗逆转录病毒疗法(ART)规模的扩大,随着疫情的进一步下降,到 2030 年,受艾滋病毒影响的夫妇中血清不一致的夫妇比例预计将增加到 70%-92%。随着疫情的出现和演变,血清不一致的稳定夫妇比例增加,然后在流行高峰期达到 2%-20%的峰值,然后随着疫情下降到 2030 年达到 0.3%-16%的水平。
血清不一致模式随疫情的演变而变化,受疫情阶段和规模的影响。最大的变化发生在艾滋病毒高流行国家。随着未来二十年抗逆转录病毒治疗规模的扩大和艾滋病毒发病率的进一步下降,预计血清不一致的稳定夫妇比例(而不是血清一致的阳性夫妇比例)将会增加。这些发现为血清不一致夫妇的干预措施的战略规划和资源分配提供了信息。