Clinical Effectiveness Unit, Royal College of Surgeons of England, London WC2A 3PE, UK.
Cambridge University Hospitals NHS Foundation Trust, Addenbrookes Hospital, Hills Road, Cambridge CB2 0QQ, UK.
BMJ. 2018 May 2;361:k1581. doi: 10.1136/bmj.k1581.
To determine the effect of surgeon specific outcome reporting in colorectal cancer surgery on risk averse clinical practice, "gaming" of clinical data, and 90 day postoperative mortality.
National cohort study.
English National Health Service hospital trusts.
111 431 patients diagnosed as having colorectal cancer from 1 April 2011 to 31 March 2015 included in the National Bowel Cancer Audit.
Public reporting of surgeon specific 90 day mortality in elective colorectal cancer surgery in England introduced in June 2013.
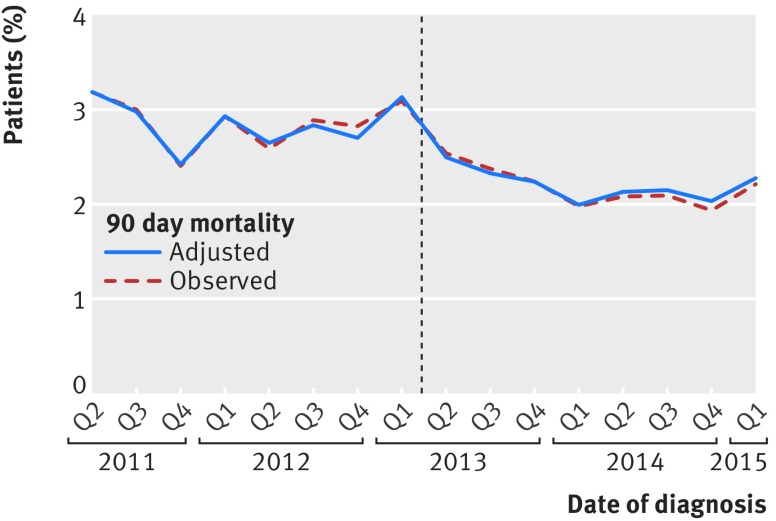
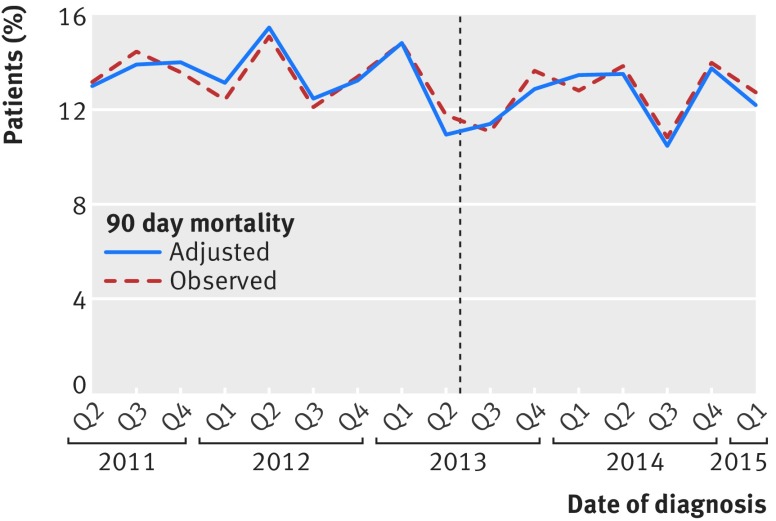
Proportion of patients with colorectal cancer who had an elective major resection, predicted 90 day mortality based on characteristics of patients and tumours, and observed 90 day mortality adjusted for differences in characteristics of patients and tumours, comparing patients who had surgery between April 2011 and June 2013 and between July 2013 and March 2015.
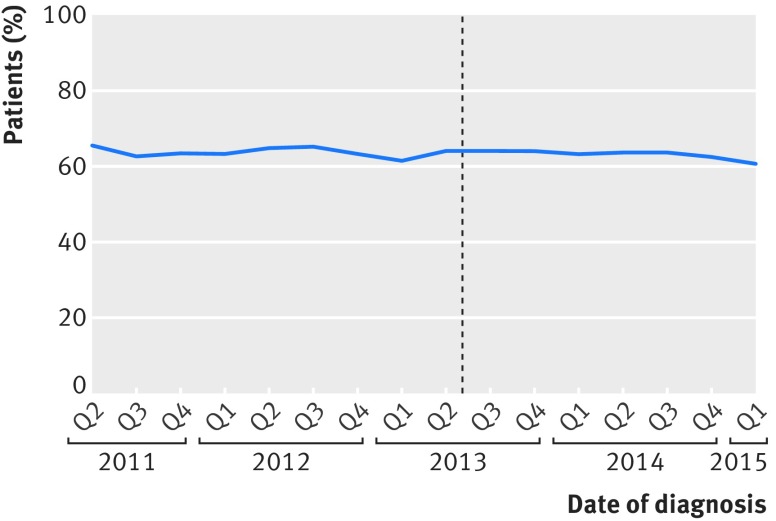
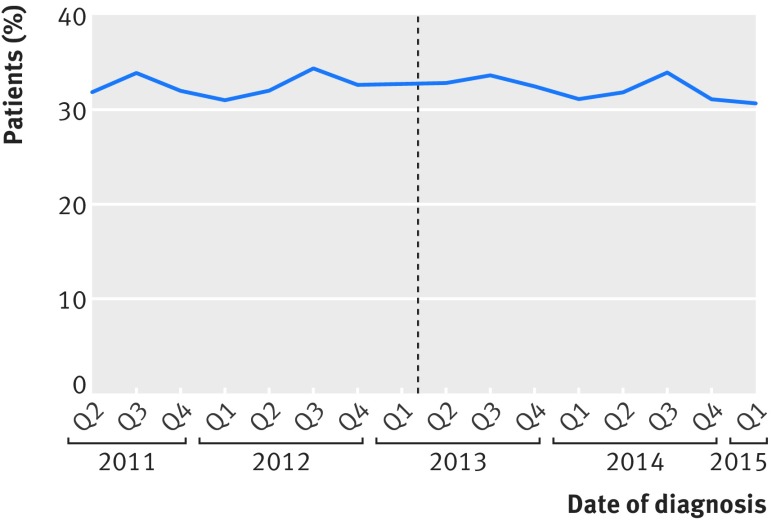
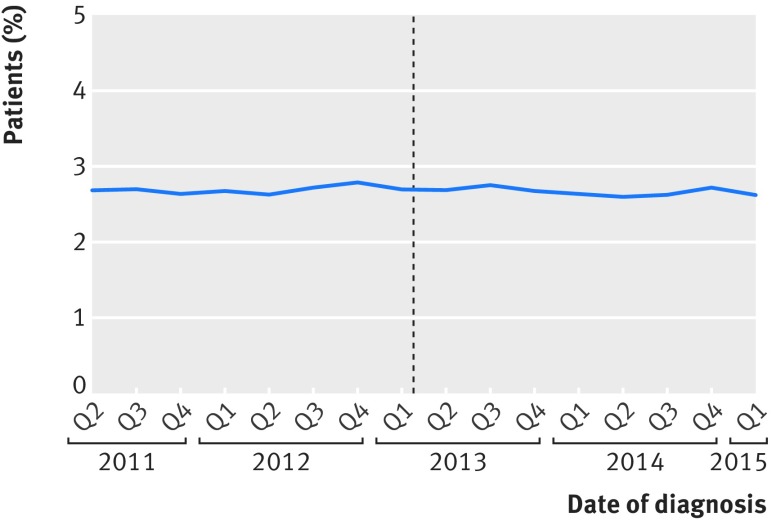
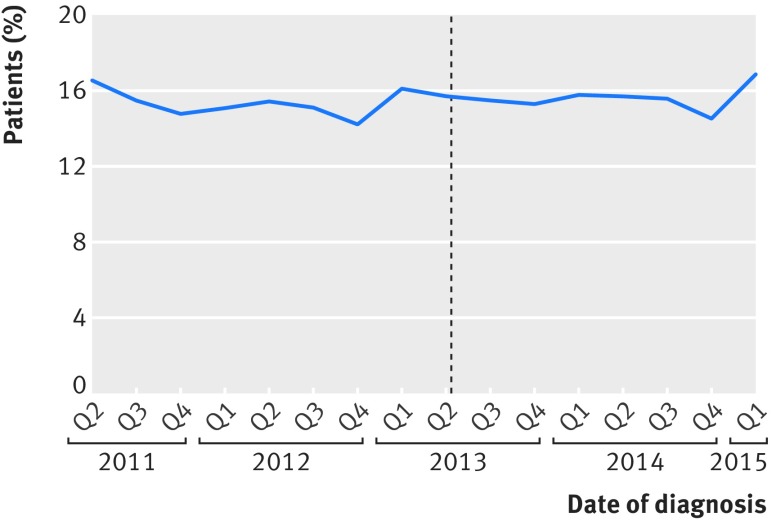
The proportion of patients with colorectal cancer undergoing major resection did not change after the introduction of surgeon specific public outcome reporting (39 792/62 854 (63.3%) before versus 30 706/48 577 (63.2%) after; P=0.8). The proportion of these major resections categorised as elective or scheduled also did not change (33 638/39 792 (84.5%) before versus 25 905/30 706 (84.4%) after; P=0.5). The predicted 90 day mortality remained the same (2.7% 2.7%; P=0.3), but the observed 90 day mortality fell (952/33 638 (2.8%) 552/25 905 (2.1%)). Change point analysis showed that this reduction was over and above the existing downward trend in mortality before the introduction of public outcome reporting (P=0.03).
This study did not find evidence that the introduction of public reporting of surgeon specific 90 day postoperative mortality in elective colorectal cancer surgery has led to risk averse clinical practice behaviour or "gaming" of data. However, its introduction coincided with a significant reduction in 90 day mortality.
确定在结直肠肿瘤外科手术中报告外科医生特定结局对规避风险的临床实践、“操纵”临床数据以及 90 天术后死亡率的影响。
全国队列研究。
英国国民保健署医院信托基金。
纳入了 2011 年 4 月 1 日至 2015 年 3 月 31 日期间国家肠道癌症审计中诊断患有结直肠肿瘤的 111431 名患者。
2013 年 6 月,在英格兰引入了外科医生特定的结直肠肿瘤择期手术 90 天死亡率的公开报告。
接受结直肠肿瘤主要切除术的患者比例,根据患者和肿瘤特征预测的 90 天死亡率,以及调整了患者和肿瘤特征差异后的观察到的 90 天死亡率,比较了 2011 年 4 月至 2013 年 6 月以及 2013 年 7 月至 2015 年 3 月之间接受手术的患者。
在引入外科医生特定的公开结局报告后,接受结直肠肿瘤主要切除术的患者比例没有变化(62854 例中的 39792 例(33.3%)之前,48577 例中的 30706 例(33.2%)之后;P=0.8)。这些主要切除术分类为选择性或计划性的比例也没有变化(39792 例中的 33638 例(84.5%)之前,30706 例中的 25905 例(84.4%)之后;P=0.5)。预测的 90 天死亡率保持不变(2.7% 2.7%;P=0.3),但观察到的 90 天死亡率下降(33638 例中的 952 例(2.8%),25905 例中的 552 例(2.1%))。转折点分析表明,这一减少超出了在引入公开结局报告之前死亡率已经存在的下降趋势(P=0.03)。
本研究没有发现证据表明,在结直肠肿瘤择期手术中报告外科医生特定的 90 天术后死亡率会导致规避风险的临床实践行为或“操纵”数据。然而,它的引入恰逢 90 天死亡率的显著下降。