Institute for Infection Prevention and Hospital Epidemiology, Medical Center - University of Freiburg, Breisacher Str. 115 B, D-79106, Freiburg, Germany.
Institute of Hygiene and Environmental Medicine, Charité University Medical Center Berlin, German National Reference Center for the Surveillance of Nosocomial Infections, Hindenburgdamm 27, D-12203, Berlin, Germany.
BMC Infect Dis. 2018 May 4;18(1):208. doi: 10.1186/s12879-018-3120-y.
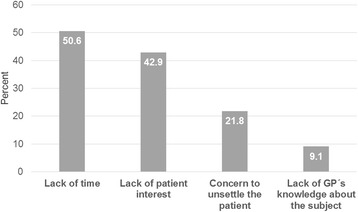
This study investigates the barriers and facilitators of the use of antibiotics in acute respiratory tract infections by general practitioners (GPs) in Germany.
A multidisciplinary team designed and pre-tested a written questionnaire addressing the topics awareness of antimicrobial resistance (7 items), use of antibiotics (9 items), guidelines/sources of information (9 items) and sociodemographic factors (7 items), using a five-point-Likert-scale ("never" to "very often"). The questionnaire was mailed by postally to 987 GPs with registered practices in eastern Germany in May 2015.
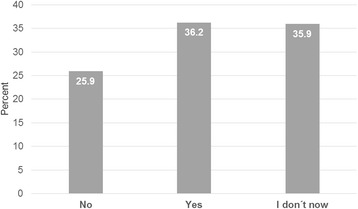
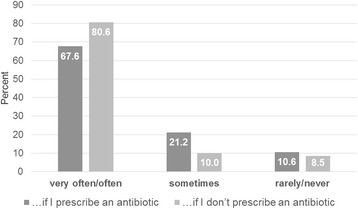
34% (340/987) of the GPs responded to this survey. Most of the participants assumed a multifactorial origin for the rise of multidrug resistant organisms. In addition, 70.2% (239/340) believed that their own prescribing behavior influenced the drug-resistance situation in their area. GPs with longer work experience (> 25 years) assumed less individual influence on drug resistance than their colleagues with less than 7 years experience as practicing physicians (Odds Ratio [OR] 0.32, 95% Confidence Interval [CI] 0.17-0.62; P < 0.001). 99.1% (337/340) of participants were familiar with the "delayed prescription" strategy to reduce antibiotic prescriptions. However, only 29.4% (74/340) answered that they apply it "often" or "very often". GPs working in rural areas were less likely than those working in urban areas to apply delayed prescription.
The knowledge on factors causing antimicrobial resistance in bacteria is good among GPs in eastern Germany. However measures to improve rational prescription are not widely implemented yet. Further efforts have to be made in order to improve rational prescription of antibiotic among GPs. Nevertheless, there is a strong awareness of antimicrobial resistance among the participating GPs.
本研究旨在探讨德国全科医生(GP)在治疗急性呼吸道感染时使用抗生素的障碍和促进因素。
一个多学科团队设计并预先测试了一份书面问卷,该问卷涉及以下主题:对抗菌药物耐药性的认识(7 项)、抗生素使用(9 项)、指南/信息来源(9 项)和社会人口因素(7 项),采用五点李克特量表(“从不”到“非常经常”)。2015 年 5 月,该问卷通过邮寄方式寄给了东德有注册执业医师的 987 名全科医生。
34%(340/987)的全科医生对这项调查做出了回应。大多数参与者认为,多药耐药菌的出现是多种因素共同作用的结果。此外,70.2%(239/340)的医生认为他们自己的处方行为影响了他们所在地区的耐药情况。工作经验超过 25 年(>25 年)的医生比工作经验少于 7 年的医生认为自己对耐药性的影响较小(比值比 [OR] 0.32,95%置信区间 [CI] 0.17-0.62;P<0.001)。99.1%(337/340)的参与者熟悉减少抗生素处方的“延迟处方”策略。然而,只有 29.4%(74/340)的医生回答他们经常或非常经常使用这种策略。在农村地区工作的医生比在城市地区工作的医生更不可能使用延迟处方。
东德的全科医生对抗生素引起细菌耐药性的因素有很好的了解。然而,改善合理处方的措施尚未得到广泛实施。为了提高全科医生合理使用抗生素的水平,还需要进一步努力。然而,参与的全科医生对抗菌药物耐药性有很强的认识。