Yi Xingyang, Lin Jing, Wang Yanfen, Zhou Ju, Zhou Qiang, Wang Chun
Department of Neurology, People's Hospital of Deyang City, Deyang 618000, Sichuan, China.
Department of Neurology, the Third Affiliated Hospital of Wenzhou Medical University, Wenzhou 325200, Zhejiang, China.
Oncotarget. 2018 Apr 13;9(28):19900-19910. doi: 10.18632/oncotarget.24945.
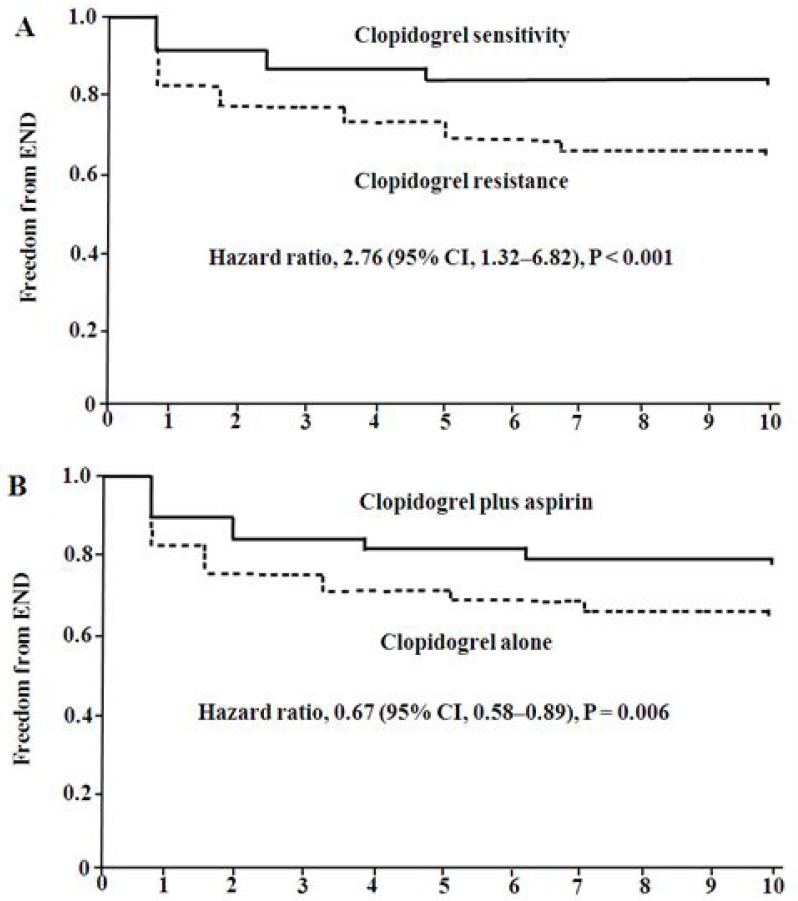
The relationship between response to clopidogrel and early neurological deterioration (END) after acute ischemic stroke (IS) is not well defined. The aim of present study was to evaluate the associations of clopidogrel resistance (CR) with END, and stratified analyze the effectiveness of clopidogrel alone and clopidogrel plus aspirin for the prevention of END.
A total of 375 patients, 144 patients were received clopidogrel alone, 231 patients took clopidogrel plus aspirin. CR occurred in 153 patients (40.8%). 95 (25.3%) patients developed END within the first 10 days. Platelet aggregation was higher on admission, and inhibition of platelet aggregation was significantly lower in patients with END than patients without END. Diabetes mellitus, CR, and clopidogrel plus aspirin were independently associated with END. Dual antiplatelet therapy with aspirin and clopidogrel can inhibit both arachidonic acid (AA)-induced and ADP-induced platelet aggregation.
This was a prospective, two-center study. A total of 375 IS patients taking clopidogrel alone or clopidogrel plus aspirin were enrolled. Platelet aggregation was measured before and after the 7-10 day treatment. CR was assessed by adenosine diphosphate (ADP)-induced platelet aggregation. The primary endpoint was END within the 10 days after admission. The secondary endpoint was a composite of recurrent ischemic stroke, myocardial infarction, and death during the 10 days after admission.
CR and END are fairly common after acute IS. CR is associated with higher risk of END. Clopidogrel plus aspirin combination therapy provides greater inhibition of platelet aggregation, and may afford protection against END.
急性缺血性卒中(IS)后氯吡格雷反应与早期神经功能恶化(END)之间的关系尚不明确。本研究旨在评估氯吡格雷抵抗(CR)与END的相关性,并分层分析单用氯吡格雷及氯吡格雷联合阿司匹林预防END的有效性。
共纳入375例患者,其中144例单用氯吡格雷,231例服用氯吡格雷联合阿司匹林。153例(40.8%)出现CR。95例(25.3%)患者在发病后10天内发生END。入院时血小板聚集率较高,发生END的患者血小板聚集抑制率显著低于未发生END的患者。糖尿病、CR以及氯吡格雷联合阿司匹林与END独立相关。阿司匹林和氯吡格雷联合抗血小板治疗可抑制花生四烯酸(AA)诱导的和二磷酸腺苷(ADP)诱导的血小板聚集。
这是一项前瞻性、双中心研究。共纳入375例单用氯吡格雷或服用氯吡格雷联合阿司匹林的IS患者。在治疗7 - 10天前后测量血小板聚集率。通过ADP诱导的血小板聚集评估CR。主要终点为入院后10天内的END。次要终点为入院后10天内复发性缺血性卒中、心肌梗死和死亡的复合终点。
急性IS后CR和END相当常见。CR与END的较高风险相关。氯吡格雷联合阿司匹林的联合治疗对血小板聚集的抑制作用更强,可能对END具有保护作用。