Department of Anesthesiology and Pain Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, 06351, Korea.
Statistics and Data Center, Samsung Medical Center, Seoul, 06351, Korea.
Sci Rep. 2018 May 8;8(1):7157. doi: 10.1038/s41598-018-25628-w.
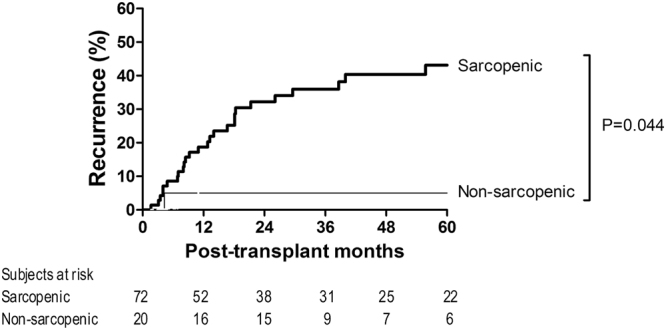
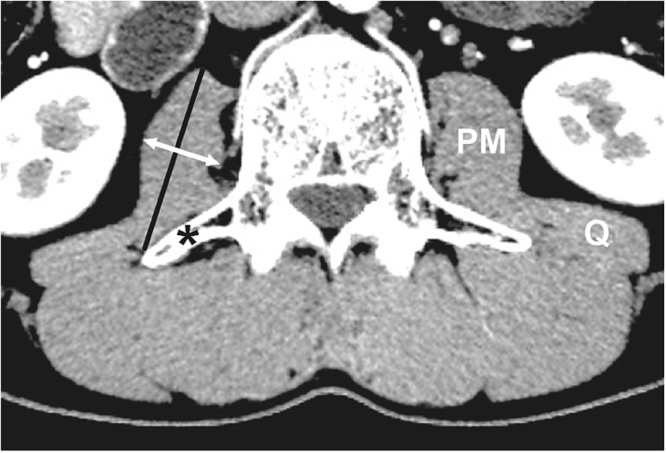
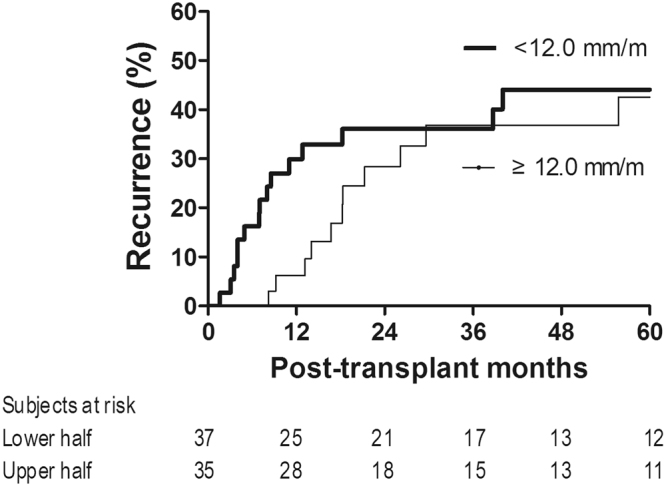
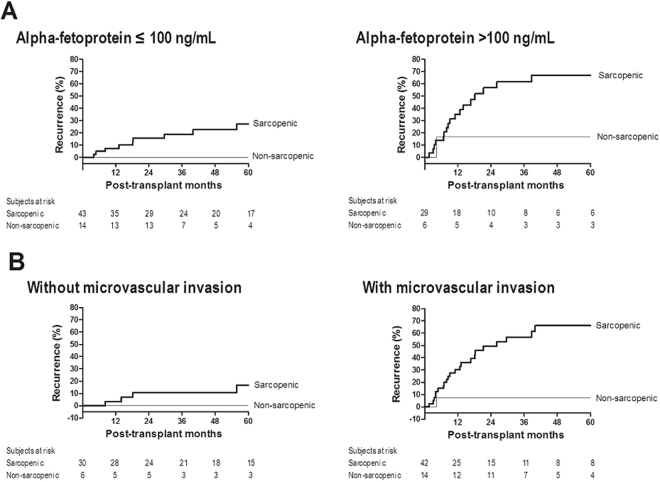
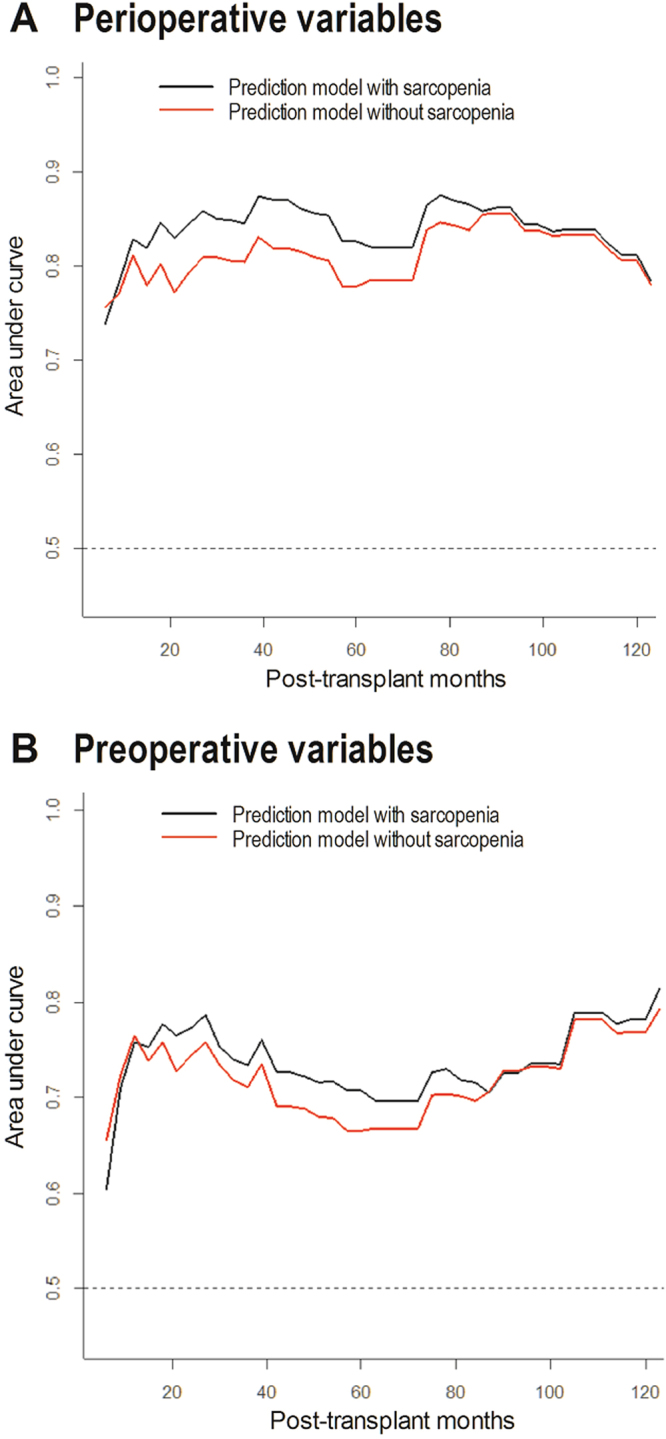
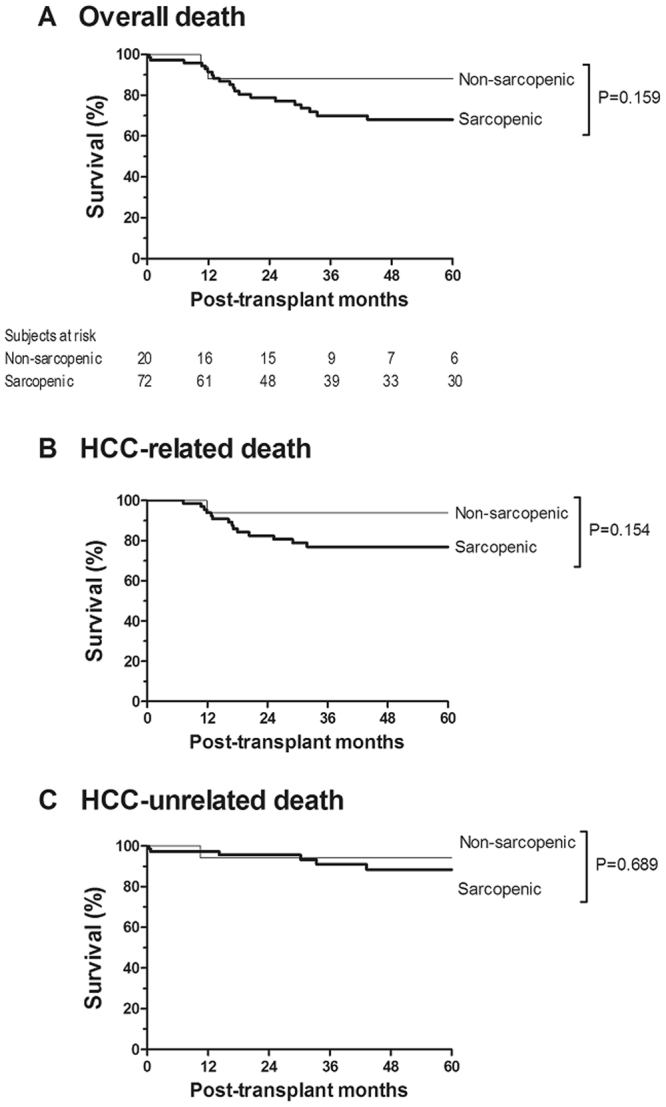
To evaluate the association between sarcopenia and tumor recurrence after living donor liver transplantation (LDLT) in patients with advanced hepatocellular carcinoma (HCC), we analyzed 92 males who underwent LDLT for treating HCC beyond the Milan criteria. Sarcopenia was defined when the height-normalized psoas muscle thickness was <15.5 mm/m at the L3 vertebra level on computed tomography based on an optimum stratification method using the Gray's test statistic. Survival analysis was performed with death as a competing risk event. The primary outcome was post-transplant HCC recurrence. The median follow-up time was 36 months. There was a 9% increase in recurrence risk per unit decrease in height-normalized psoas muscle thickness. Twenty-six (36.1%) of 72 sarcopenic recipients developed HCC recurrence, whereas only one (5.0%) of 20 non-sarcopenic recipients developed HCC recurrence. Recurrence risk was greater in sarcopenic patients in univariable analysis (hazard ratio [HR] = 8.06 [1.06-16.70], p = 0.044) and in multivariable analysis (HR = 9.49 [1.18-76.32], p = 0.034). Greater alpha-fetoprotein and microvascular invasion were also identified as independent risk factors. Incorporation of sarcopenia improved the model fitness and prediction power of the estimation model. In conclusion, sarcopenia appears to be one of the important host factors modulating tumor recurrence risk after LDLT for advanced HCC.
为了评估在超出米兰标准的肝细胞癌(HCC)患者中,肌肉减少症与活体肝移植(LDLT)后肿瘤复发之间的关联,我们分析了 92 名接受 LDLT 治疗的男性 HCC 患者。在 CT 上基于 Gray 检验统计量的最佳分层方法,当第 3 腰椎水平的身高归一化腰大肌厚度<15.5mm/m 时定义为肌肉减少症。采用死亡作为竞争风险事件进行生存分析。主要结局是移植后 HCC 复发。中位随访时间为 36 个月。身高归一化腰大肌厚度每减少一个单位,复发风险增加 9%。72 名肌肉减少症受者中有 26 名(36.1%)发生 HCC 复发,而 20 名非肌肉减少症受者中仅有 1 名(5.0%)发生 HCC 复发。单变量分析中肌肉减少症患者的复发风险更高(风险比[HR] = 8.06 [1.06-16.70],p = 0.044),多变量分析中也如此(HR = 9.49 [1.18-76.32],p = 0.034)。较高的甲胎蛋白和微血管侵犯也被确定为独立的危险因素。纳入肌肉减少症可提高模型拟合度和预测能力。总之,肌肉减少症似乎是调节晚期 HCC 患者 LDLT 后肿瘤复发风险的重要宿主因素之一。