Division of Experimental Medicine and Immunotherapeutics, Department of Medicine, University of Cambridge, Cambridge, UK.
Cambridge Clinical Trials Unit, Cambridge, UK.
BMJ Open. 2018 May 9;8(5):e022859. doi: 10.1136/bmjopen-2018-022859.
Vasopressin stimulates cyst growth in autosomal dominant polycystic kidney disease (ADPKD) leading to enlarged kidneys, hypertension and renal failure. Vasopressin receptor blockade slows disease progression. Physiological suppression of vasopressin secretion through high water (HW) intake could achieve a similar effect, necessitating a definitive large-scale trial of HW intake in ADPKD. The objective of the DRINK trial is to answer the key design and feasibility questions required to deliver a successful definitive water intake trial.
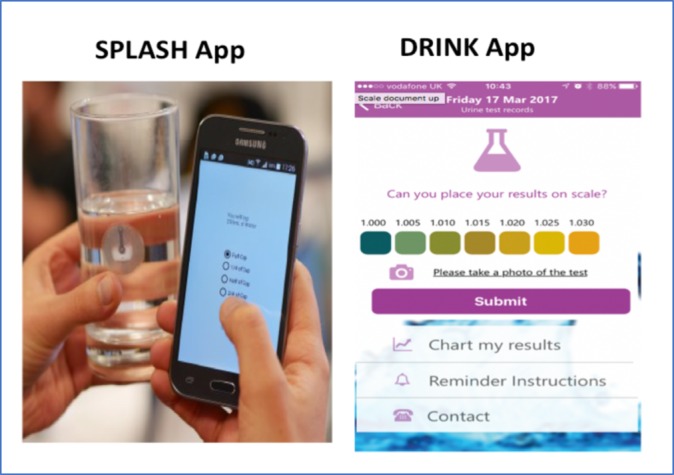
We describe the design of a single-centre, open-label, prospective, randomised controlled trial. The "etermining feasibility of andomisation to high vs. ad libitum water take in Polycystic idney Disease" (DRINK) trial aims to enrol 50 patients with ADPKD, over the age of 16 years with an estimated glomerular filtration rate (eGFR) ≥20 mL/min/1.73 m. Participants will be randomised 1:1 to HW intake based on an individualised water intake prescription, or to ad libitum (AW) water intake. The HW group will aim for a dilute urine (urine osmolality ≤270 mOsm/kg) as a surrogate marker of vasopressin suppression, and those in the AW group will target more concentrated urine. Participants will have an 8-week treatment period, and will be seen at weeks 0, 2, 4 and 8, undergoing assessments of fluid status, renal function and serum and urine osmolalities. They will receive dietary advice, and self-monitor urine specific gravity and fluid intake. The trial employs smartphone technology to permit home monitoring and remote direct data capture. The primary feasibility end points are recruitment rate and separation between arms in measured urinary osmolality. Key secondary assessments include acceptability, adherence, health-related quality of life, acute effects of HW intake on measured (Cr-EDTA) and eGFR and ADPKD-related pain.
Ethical approval was awarded by the East of England Essex Research Ethics Committee (16/EE/0026). The results of DRINK will be submitted to peer-reviewed journals, and presented to patients via the PKD Charity.
NCT02933268 and ISCRTN16794957.
血管加压素刺激常染色体显性多囊肾病(ADPKD)中的囊肿生长,导致肾脏增大、高血压和肾衰竭。血管加压素受体阻断可减缓疾病进展。通过高水(HW)摄入来抑制血管加压素分泌的生理作用可能会产生类似的效果,因此需要在 ADPKD 中进行大规模的 HW 摄入确定性试验。DRINK 试验的目的是回答在 ADPKD 中进行成功的 HW 摄入随机试验所需的关键设计和可行性问题。
我们描述了一项单中心、开放标签、前瞻性、随机对照试验的设计。“确定在常染色体显性多囊肾病中进行高 vs. 随意水摄入随机化的可行性”(DRINK)试验旨在招募 50 名年龄在 16 岁以上、估算肾小球滤过率(eGFR)≥20mL/min/1.73m 的 ADPKD 患者。参与者将按 1:1 随机分为 HW 摄入组和 AW 摄入组(随意水摄入)。HW 组将以尿液渗透压≤270mOsm/kg 为抑制血管加压素的替代标志物,目标是稀释尿液,而 AW 组将以浓缩尿液为目标。参与者将接受为期 8 周的治疗,在第 0、2、4 和 8 周时进行液体状态、肾功能和血清及尿液渗透压的评估。他们将接受饮食建议,并自行监测尿比重和液体摄入量。该试验采用智能手机技术,允许家庭监测和远程直接数据采集。主要可行性终点是招募率和测量尿渗透压的两个手臂之间的分离。关键次要评估包括可接受性、依从性、健康相关生活质量、HW 摄入对测量(Cr-EDTA)和 eGFR 的急性影响以及 ADPKD 相关疼痛。
伦理批准由东英格兰埃塞克斯研究伦理委员会授予(16/EE/0026)。DRINK 的结果将提交给同行评议期刊,并通过 PKD 慈善机构向患者展示。
NCT02933268 和 ISCRTN16794957。