Baylor College of Medicine, Houston, TX.
University of Connecticut School of Pharmacy, Storrs, CT.
Acad Emerg Med. 2018 Sep;25(9):995-1003. doi: 10.1111/acem.13451. Epub 2018 Jun 11.
Hospitalization for low-risk pulmonary embolism (PE) is common, expensive, and of questionable benefit.
The objective was to determine if low-risk PE patients discharged from the emergency department (ED) on rivaroxaban require fewer hospital days compared to standard of care (SOC).
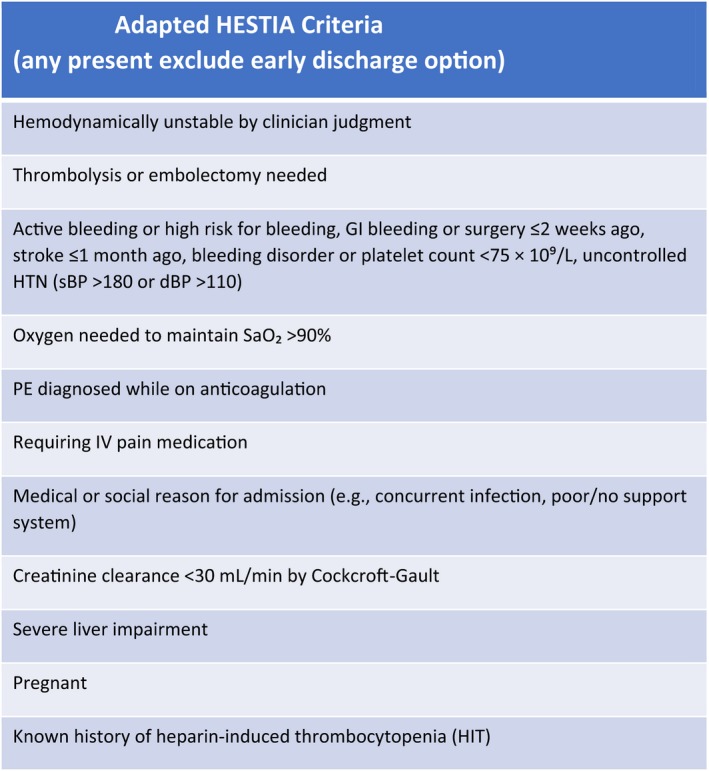
Multicenter, open-label randomized trial in low-risk PE defined by Hestia criteria. Adult subjects were randomized to early ED discharge on rivaroxaban or SOC. Primary outcome was total number of initial hospital hours, plus hours of hospitalization for bleeding or venous thromboembolism (VTE), 30 days after randomization. A 90-day composite safety endpoint was defined as major bleeding, clinically relevant nonmajor bleeding, and mortality.
Of 114 randomized subjects, 51 were early discharge and 63 were SOC. Of 112 (98.2%) receiving at least one dose of study drug, 99 (86.8%) completed the study. Initial hospital LOS was 4.8 hours versus 33.6 hours, with a mean difference of -28.8 hours (95% confidence interval [CI] = -42.55 to -15.12 hours) for early discharge versus SOC, respectively. At 90 days, mean total hospital days (for any reason) were less for early discharge than SOC, 19.2 hours versus 43.2 hours, with a mean difference of 26.4 hours (95% CI = -46.97 to -3.34 hours). At 90 days, there were no bleeding events, recurrent VTE, or deaths. The composite safety endpoint was similar in both groups, with a difference in proportions of 0.005 (95% CI = -0.18 to 0.19). Total costs were $1,496 for early discharge and $4,234 for SOC, with a median difference of $2,496 (95% CI = -$2,999 to -$2,151).
Low-risk ED PE patients receiving early discharge on rivaroxaban have similar outcomes to SOC, but fewer total hospital days and lower costs over 30 days.
低危肺栓塞(PE)患者住院治疗较为常见,费用昂贵,且疗效存在争议。
本研究旨在确定从急诊科(ED)出院的低危 PE 患者接受利伐沙班治疗与标准治疗(SOC)相比是否需要更少的住院天数。
这是一项多中心、开放性标签、低危 PE 患者随机试验,采用 Hestia 标准进行定义。成年受试者被随机分为利伐沙班组和 SOC 组,在 ED 早期出院。主要结局为随机分组后 30 天内初始住院总时间,加上因出血或静脉血栓栓塞(VTE)住院的时间。90 天复合安全性终点定义为大出血、临床相关非大出血和死亡率。
在 114 名随机受试者中,51 名进行早期出院,63 名进行 SOC。112 名(98.2%)受试者至少接受一剂研究药物治疗,其中 99 名(86.8%)完成了研究。早期出院组的初始住院 LOS 为 4.8 小时,SOC 组为 33.6 小时,分别相差-28.8 小时(95%置信区间[CI]:-42.55 至-15.12 小时)。90 天时,早期出院组的总住院天数(任何原因)均少于 SOC 组,分别为 19.2 小时和 43.2 小时,相差 26.4 小时(95%CI:-46.97 至-3.34 小时)。90 天时,两组均无出血事件、复发性 VTE 或死亡。两组的复合安全性终点相似,比例差异为 0.005(95%CI:-0.18 至 0.19)。早期出院组总费用为 1496 美元,SOC 组为 4234 美元,中位数相差 2496 美元(95%CI:-2999 美元至-2151 美元)。
接受利伐沙班早期出院的低危 ED PE 患者与 SOC 相比具有相似的结局,但总住院天数更少,30 天内成本更低。