Orthodontic Graduate Program, School of Dentistry, Edmonton Clinic Health Academy, University of Alberta, 11405-87 Ave, Edmonton, AB, T6G 1C9, Canada.
Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, AB, Canada.
BMC Med Res Methodol. 2018 May 18;18(1):42. doi: 10.1186/s12874-018-0491-0.
Recent methodologic evidence suggests that lack of blinding in randomized trials can result in under- or overestimation of the treatment effect size. The objective of this study is to quantify the extent of bias associated with blinding in randomized controlled trials of oral health interventions.
We selected all oral health meta-analyses that included a minimum of five randomized controlled trials. We extracted data, in duplicate, related to nine blinding-related criteria, namely: patient blinding, assessor blinding, care-provider blinding, investigator blinding, statistician blinding, blinding of both patients and assessors, study described as "double blind", blinding of patients, assessors, and care providers concurrently, and the appropriateness of blinding. We quantified the impact of bias associated with blinding on the magnitude of effect size using a two-level meta-meta-analytic approach with a random effects model to allow for intra- and inter-meta-analysis heterogeneity.
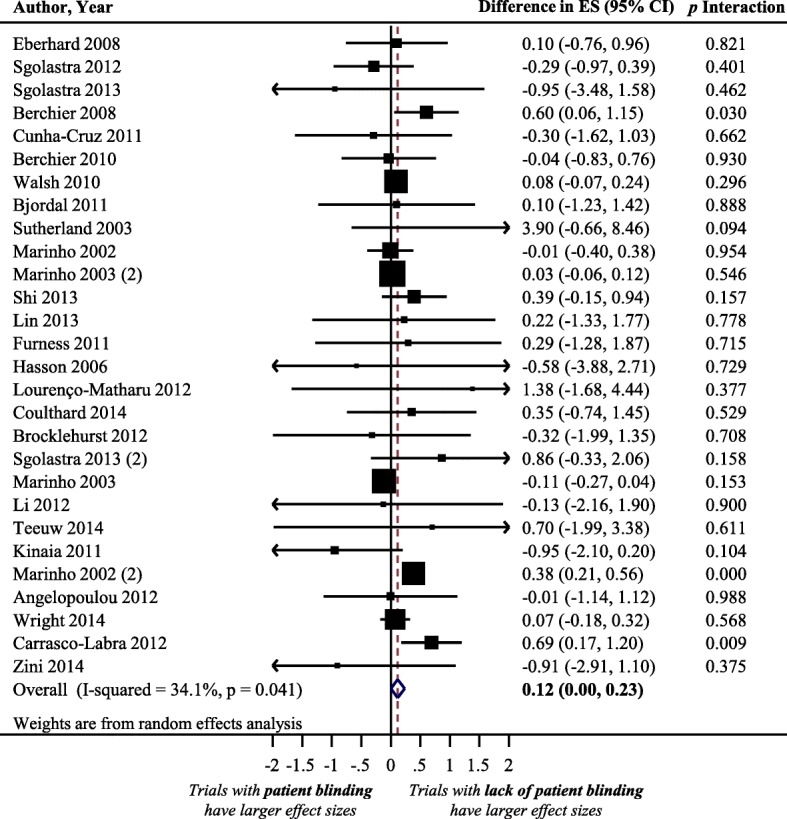
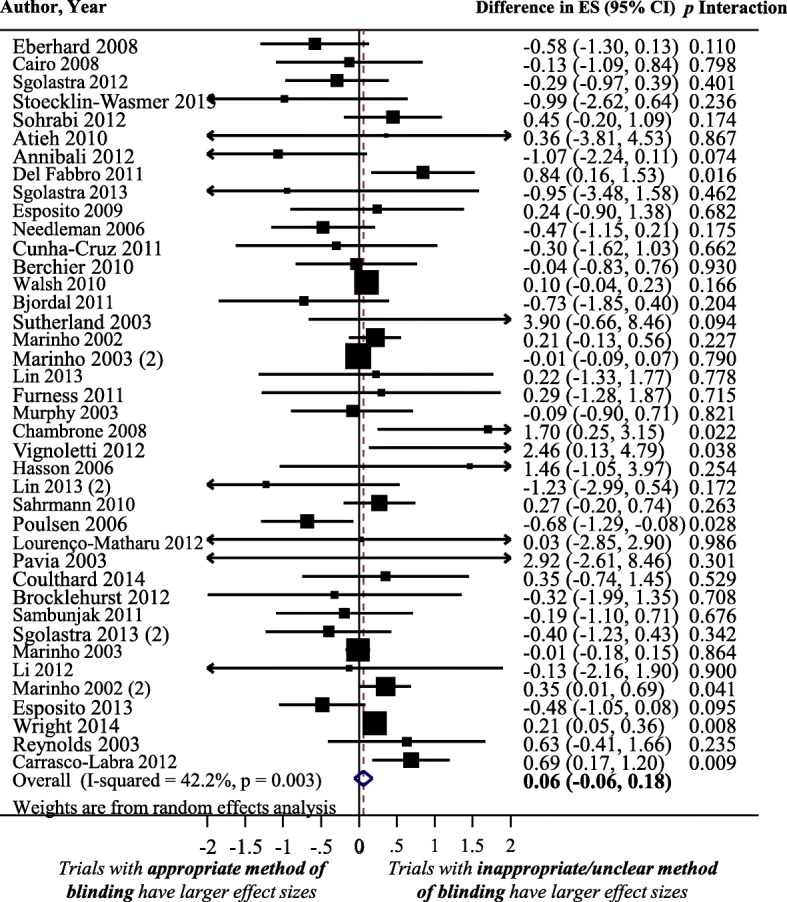
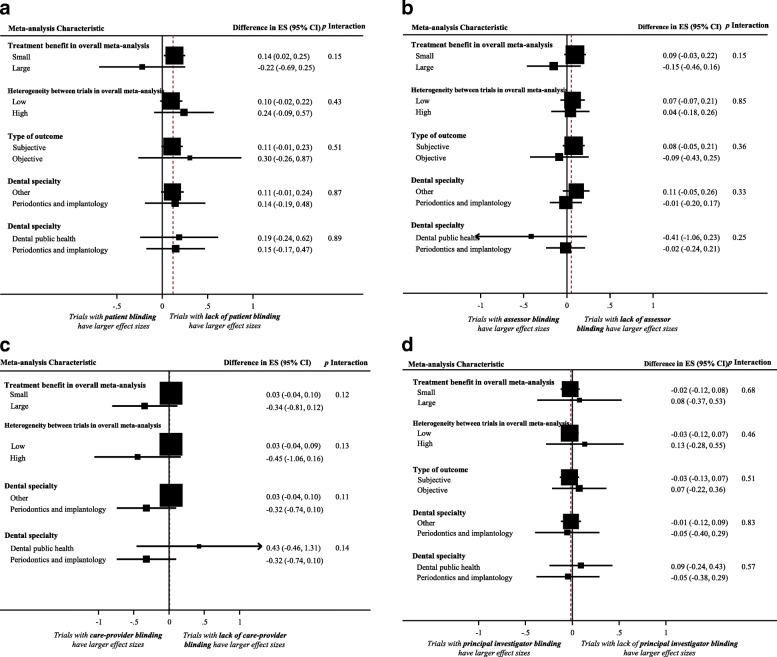
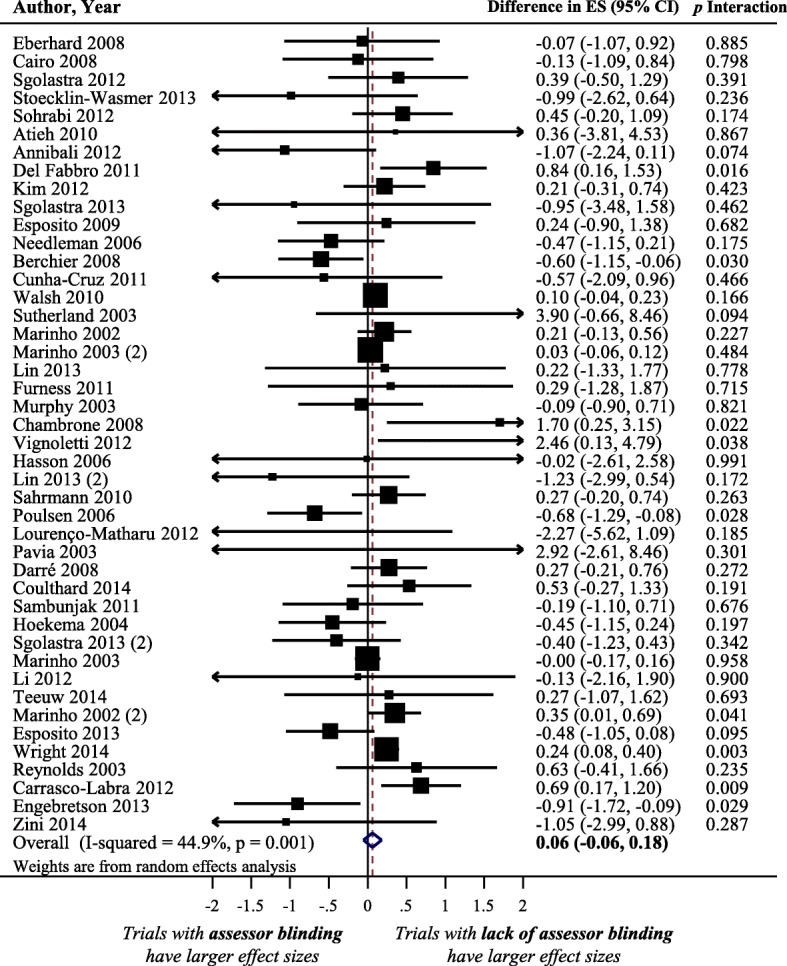
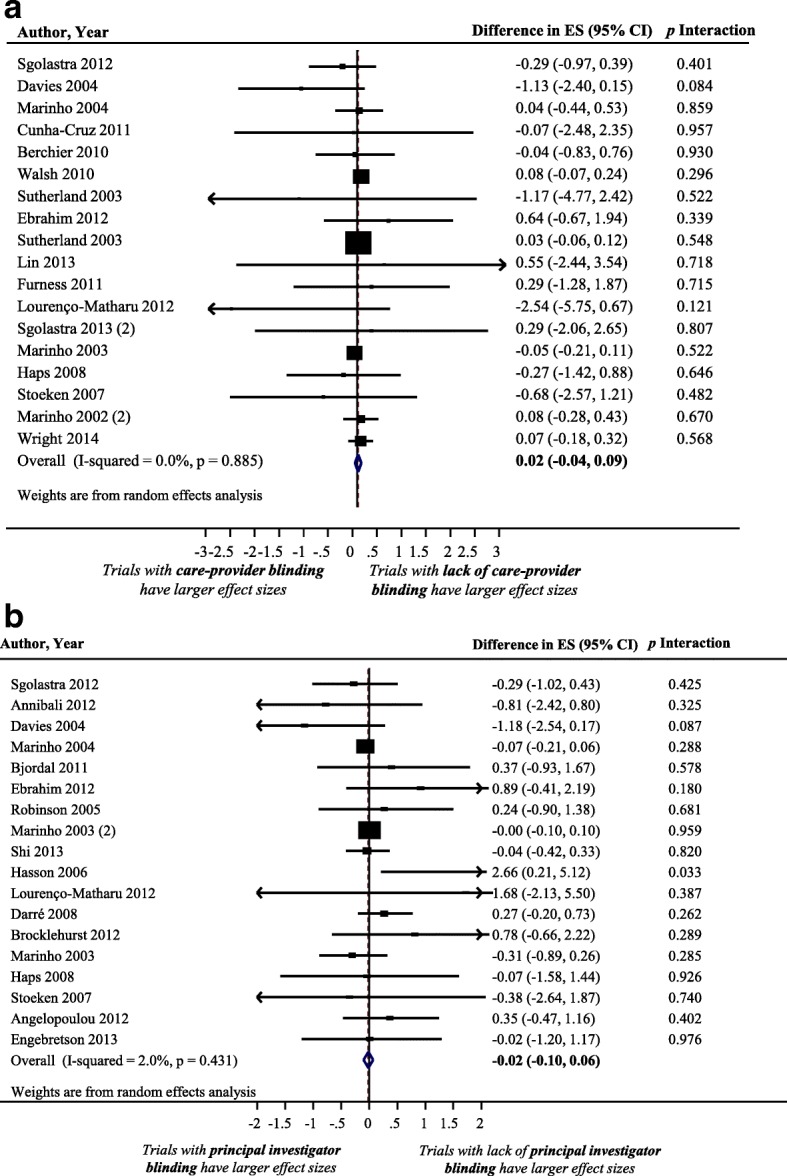
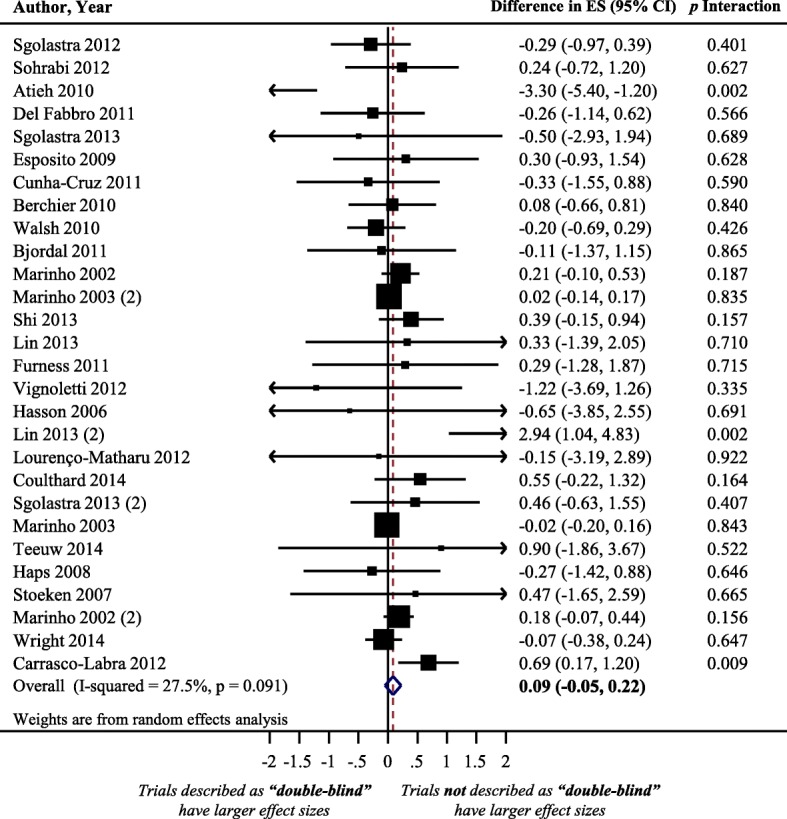
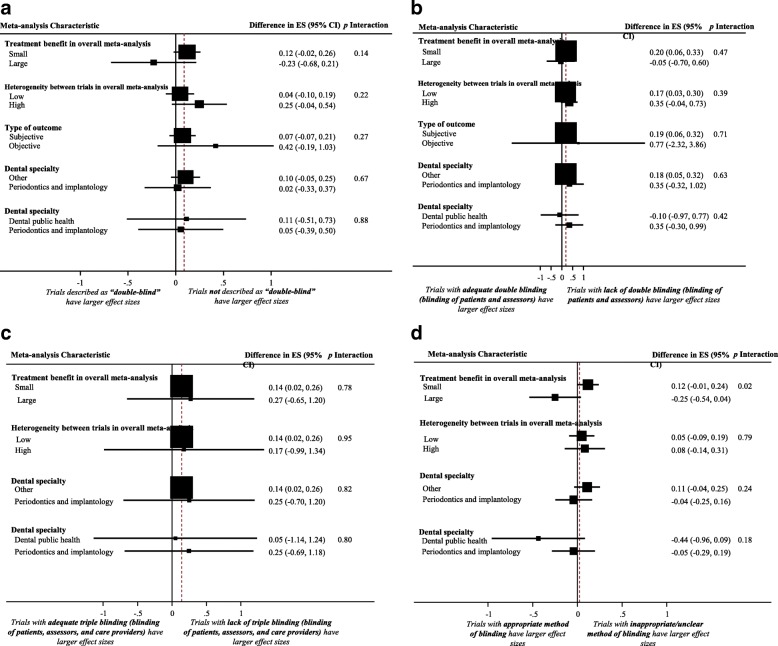
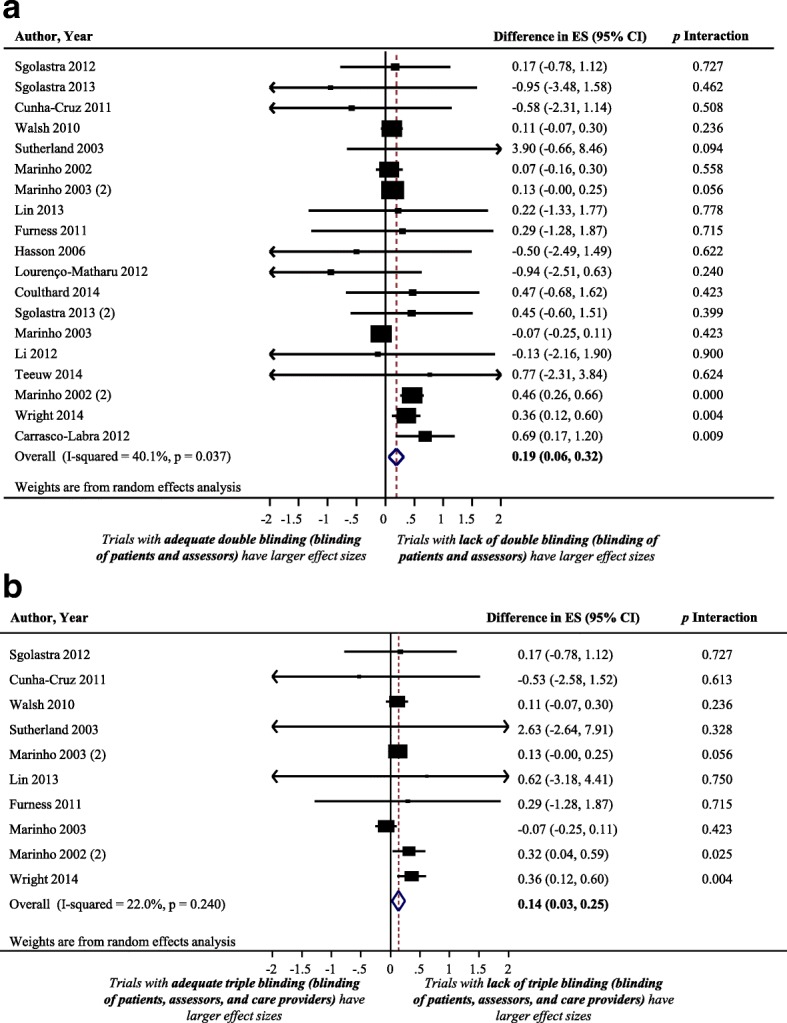
We identified 540 randomized controlled trials, included in 64 meta-analyses, analyzing data from 137,957 patients. We identified significantly larger treatment effect size estimates in trials that had inadequate patient blinding (difference in treatment effect size = 0.12; 95% CI: 0.00 to 0.23), lack of blinding of both patients and assessors (difference = 0.19; 95% CI: 0.06 to 0.32), and lack of blinding of patients, assessors, and care-providers concurrently (difference = 0.14; 95% CI: 0.03 to 0.25). In contrast, assessor blinding (difference = 0.06; 95% CI: -0.06 to 0.18), caregiver blinding (difference = 0.02; 95% CI: -0.04 to 0.09), principal-investigator blinding (difference = - 0.02; 95% CI: -0.10 to 0.06), describing a trial as "double-blind" (difference = 0.09; 95% CI: -0.05 to 0.22), and lack of an appropriate method of blinding (difference = 0.06; 95% CI: -0.06 to 0.18) were not associated with over- or underestimated treatment effect size.
We found significant differences in treatment effect size estimates between oral health trials based on lack of patient and assessor blinding. Treatment effect size estimates were 0.19 and 0.14 larger in trials with lack of blinding of both patients and assessors and blinding of patients, assessors, and care-providers concurrently. No significant differences were identified in other blinding criteria. Investigators of oral health systematic reviews should perform sensitivity analyses based on the adequacy of blinding in included trials.
最近的方法学证据表明,随机试验中缺乏盲法可能导致对治疗效果大小的低估或高估。本研究的目的是量化口腔健康干预措施的随机对照试验中与盲法相关的偏倚程度。
我们选择了所有包含至少五项随机对照试验的口腔健康荟萃分析。我们提取了与九个与盲法相关的标准相关的数据,即:患者盲法、评估者盲法、提供者盲法、研究者盲法、统计师盲法、患者和评估者双盲、研究描述为“双盲”、患者盲法、评估者盲法和提供者盲法同时进行、以及盲法的适当性。我们使用两水平元分析荟萃分析方法和随机效应模型来量化与盲法相关的偏倚对效应大小的影响,以允许内和间荟萃分析异质性。
我们确定了 540 项随机对照试验,这些试验包含在 64 项荟萃分析中,分析了来自 137957 名患者的数据。我们发现,在缺乏患者盲法(治疗效果差异=0.12;95%CI:0.00 至 0.23)、缺乏患者和评估者双盲(差异=0.19;95%CI:0.06 至 0.32)以及缺乏患者、评估者和护理提供者同时盲法(差异=0.14;95%CI:0.03 至 0.25)的试验中,治疗效果估计值显著更大。相比之下,评估者盲法(差异=0.06;95%CI:-0.06 至 0.18)、护理提供者盲法(差异=0.02;95%CI:-0.04 至 0.09)、主要研究者盲法(差异=-0.02;95%CI:-0.10 至 0.06)、将试验描述为“双盲”(差异=0.09;95%CI:-0.05 至 0.22)以及缺乏适当的盲法方法(差异=0.06;95%CI:-0.06 至 0.18)与过高或过低的治疗效果估计值无关。
我们发现,基于患者和评估者盲法的缺失,口腔健康试验的治疗效果估计值存在显著差异。在缺乏患者和评估者双盲以及同时缺乏患者、评估者和护理提供者盲法的试验中,治疗效果估计值分别增加了 0.19 和 0.14。在其他盲法标准中没有发现显著差异。口腔健康系统评价的研究者应根据纳入试验的盲法质量进行敏感性分析。