Department of Obstetrics and Gynecology (OB/GYN), Paracelsus Medical University, Muellner Hauptstr. 48, A-5020, Salzburg, Austria.
Paracelsus Medical University, Salzburg, Austria.
BMC Pregnancy Childbirth. 2018 May 18;18(1):176. doi: 10.1186/s12884-018-1815-0.
Spontaneous vaginal twin delivery after 32nd week of gestation is safe when first twin presenting cephalic. Aim of this study is to identify obstetric factors influencing the condition of second twin and to verify whether non-cephalic presentation and vaginal breech delivery of the second twin is safe.
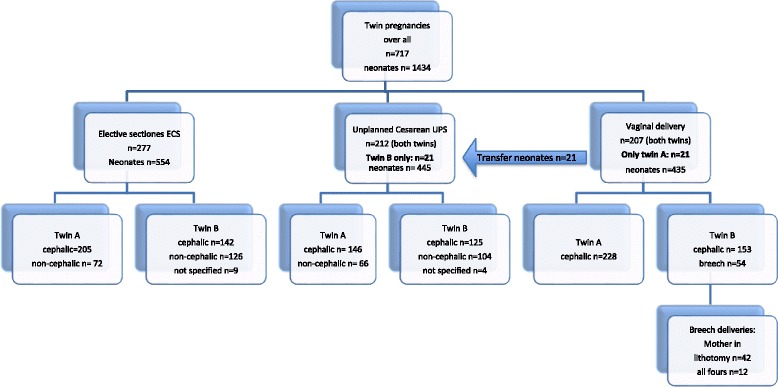
This is a retrospective case controlled cohort study of 717 uncomplicated twin deliveries ≥32 + 0 weeks of gestation from 2005 to 2014 in two tertiary perinatal centers. Obstetric parameters were evaluated in three groups with descriptive, univariate logistic regression analysis for perinatal outcome of second twins.
The three groups included twins delivered by elective cesarean section ECS (n = 277, 38.6%), by unplanned cesarean section UPC (n = 233, 32.5%) and vaginally (n = 207, 28.9%). Serious adverse fetal outcome is rare and we found no differences between the groups. Second twins after ECS had significant better umbilical artery UA pH (p < 0.001) and better Apgar compared to UPC (p = 0.002). Variables for a fetal population "at risk" for adverse neonatal outcome after vaginal delivery (UA pH < 7.20, Apgar 5´ < 9) were associated with higher gestational age (p = 0.001), longer twin-twin interval (p = 0.05) and vacuum extraction of twin A (p = 0.04). Non-cephalic presentation of second twins was not associated (UA pH < 7.20 OR 1.97, CI 95% 0.93-4.22, p = 0.07, Apgar 5´ < 9 OR 1.63, CI 95% 0.70-3.77, p = 0.25, Transfer to neonatal intermediate care unit p = 0.48). Twenty-one second twins (2,9%) were delivered by cesarean section following vaginal delivery of the first twin. Even though non-cephalic presentation was overrepresented in this subgroup, outcome variables were not significantly different compared to cephalic presentation.
Even though elective cesarean means reduced stress for second twins this seems not to be clinically relevant. Non-cephalic presentation of the second twin does not significantly influence the perinatal outcome of the second twin but might be a risk factor for vaginal-cesarean birth.
妊娠 32 周后,当第一胎为头位时,阴道自然分娩双胞胎是安全的。本研究旨在确定影响第二胎情况的产科因素,并验证第二胎非头位和阴道臀位分娩是否安全。
这是一项回顾性病例对照队列研究,纳入了 2005 年至 2014 年在两个三级围产中心分娩的 717 例≥32+0 周的单绒毛膜双胎妊娠。对三组孕妇的产科参数进行描述性、单变量逻辑回归分析,以评估第二胎的围产结局。
三组包括经择期剖宫产(ECS)分娩的双胞胎(n=277,38.6%)、经计划性剖宫产(UPC)分娩的双胞胎(n=233,32.5%)和经阴道分娩的双胞胎(n=207,28.9%)。严重的胎儿不良结局很少见,三组间无差异。与 UPC 组相比,ECS 组的第二胎脐动脉 pH 值(p<0.001)和 Apgar 评分(p=0.002)明显更好。与阴道分娩新生儿不良结局相关的(脐动脉 pH 值<7.20,Apgar 评分 5 分钟<9)的胎儿不良结局高危因素包括较高的胎龄(p=0.001)、较长的双胎间隔(p=0.05)和第一胎的真空吸引(p=0.04)。第二胎非头位与(脐动脉 pH 值<7.20 的比值比 1.97,95%置信区间 0.93-4.22,p=0.07,Apgar 评分 5 分钟<9 的比值比 1.63,95%置信区间 0.70-3.77,p=0.25,转新生儿中间护理病房的比值比 1.48,95%置信区间 0.70-3.08,p=0.30)、非头位向头位的转化率(p=0.37)、新生儿入住新生儿重症监护病房的比值比(p=0.14)均无关。21 例第二胎(2.9%)在第一胎阴道分娩后行剖宫产术。尽管该亚组中非头位分娩的比例较高,但与头位分娩相比,围产结局变量并无显著差异。
尽管选择性剖宫产对第二胎的压力较小,但这似乎在临床上并无意义。第二胎非头位并不显著影响第二胎的围产结局,但可能是阴道-剖宫产分娩的危险因素。