Department of Nephrology and Rheumatology, Iwate Prefectural Central Hospital, 1-4-1, Morioka, 020-0066, Japan.
Department of Nephrology, Kumamoto University School of Medicine, Honjyo 1-1-1, Chuo-Ku, Kumamoto, 860-8556, Japan.
BMC Nephrol. 2018 May 23;19(1):122. doi: 10.1186/s12882-018-0916-3.
Liddle's syndrome is a rare monogenic form of hypertension caused by truncating or missense mutations in the C termini of the epithelial sodium channel (ENaC) β or γ subunits. Patients with this syndrome present with early onset of hypertension, hypokalemia, metabolic alkalosis, hyporeninemia and hypoaldosteronism, and a potassium-sparing diuretics (triamterene or amiloride) can drastically improves the disease condition. Although elderly patients having these characteristics were considered to have Liddle's syndrome or Liddle's-like syndrome, no previous report has indicated that Liddle's-like syndrome could be caused by nephrotic syndrome of primary glomerular disease, which is characterized by urinary excretion of > 3 g of protein/day plus edema and hypoalbuminemia, or has explained how the activity function of ENaC could be affected in the setting of high proteinuria.
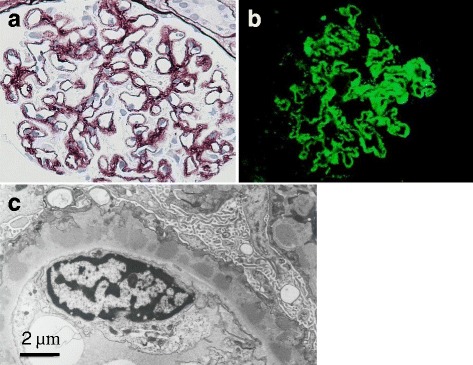
A 65-year-old Japanese man presented with nephrotic syndrome. He had no remarkable family history, but had a medical history of hypertension and hyperlipidemia. On admission, hypertension, spironolactone-resistant hypokalemia (2.43 mEq/l), hyporeninemic hypoaldosteronism, and metabolic alkalosis, which suggested Liddle's syndrome, were observed. Treatment with triamterene together with a steroid for nephrotic syndrome resulted in rapid and remarkable effective on improvements of hypertension, hypokalemia, and edema of the lower extremities. Renal biopsy revealed membranous nephropathy (MN) as the cause of nephrotic syndrome, and advanced gastric cancer was identified on screening examination for cancers that could be associated with the development of MN. After total gastrectomy, triamterene was not required and proteinuria decreased. A mutation in the β or γ subunits of the ENaC gene was not identified.
We reported for the first time a case of Liddle's-like syndrome associated with nephrotic syndrome secondary to MN. Aberrant activation of ENaC was suggested transient during the period of high proteinuria, and the activation was reversible with a decrease in proteinuria.
Liddle 综合征是一种罕见的单基因遗传性高血压,由上皮钠通道(ENaC)β或γ亚基的 C 末端截断或错义突变引起。患有这种综合征的患者表现为高血压、低钾血症、代谢性碱中毒、肾素减少和醛固酮减少,保钾利尿剂(螺内酯或阿米洛利)可显著改善病情。尽管有这些特征的老年患者被认为患有 Liddle 综合征或 Liddle 样综合征,但以前没有报道表明 Liddle 样综合征可能由原发性肾小球疾病的肾病综合征引起,其特征是每日尿蛋白排泄量>3g,伴水肿和低白蛋白血症,也没有解释在大量蛋白尿的情况下 ENaC 的活性功能如何受到影响。
一名 65 岁日本男性因肾病综合征就诊。他没有明显的家族史,但有高血压和高脂血症病史。入院时,观察到高血压、螺内酯抵抗性低钾血症(2.43mEq/l)、低肾素性醛固酮减少症和代谢性碱中毒,提示为 Liddle 综合征。肾病综合征给予螺内酯加类固醇治疗,迅速显著改善了高血压、低钾血症和下肢水肿。肾活检显示膜性肾病(MN)为肾病综合征的病因,筛查检查发现与 MN 发生相关的胃癌晚期。全胃切除术后,不再需要螺内酯,蛋白尿减少。未发现 ENaC 的β或γ亚基基因突变。
我们首次报道了一例与 MN 继发肾病综合征相关的 Liddle 样综合征。在高蛋白质尿期间,ENaC 的异常激活被认为是短暂的,并且随着蛋白尿的减少,激活是可逆的。