Unidade de Xenética, Departamento de Anatomía Patolóxica e Ciencias Forenses, Instituto de Ciencias Forenses, Facultade de Medicina, Universidade de Santiago de Compostela, Galicia, Spain.
GenPoB Research Group, Instituto de Investigaciones Sanitarias (IDIS), Hospital Clínico Universitario de Santiago (SERGAS), Galicia, Spain.
Sci Rep. 2018 May 23;8(1):8043. doi: 10.1038/s41598-018-26239-1.
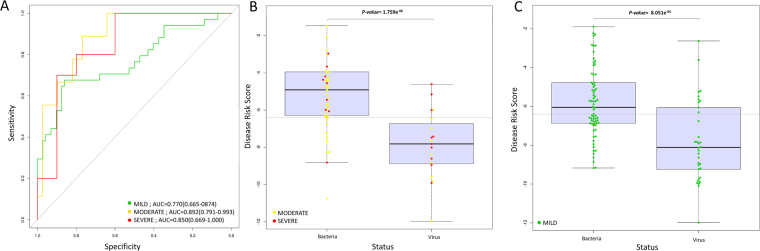
Recently, a biomarker signature consisting of 2-transcript host RNAs was proposed for discriminating bacterial from viral infections in febrile children. We evaluated the performance of this signature in a different disease scenario, namely a cohort of Mexican children (n = 174) suffering from acute diarrhea of different infectious etiologies. We first examined the admixed background of the patients, indicating that most of them have a predominantly Native American genetic ancestry with a variable amount of European background (ranging from 0% to 57%). The results confirm that the RNA test can discriminate between viral and bacterial causes of infection (t-test; P-value = 6.94×10; AUC = 80%; sensitivity: 68% [95% CI: 55%-79%]; specificity: 84% [95% CI: 78%-90%]), but the strength of the signal differs substantially depending on the causal pathogen, with the stronger signal being that of Shigella (P-value = 3.14 × 10; AUC = 89; sensitivity: 70% [95% CI: 57%-83%]; specificity: 100% [95% CI: 100%-100%]). The accuracy of this test improves significantly when excluding mild cases (P-value = 2.13 × 10; AUC = 85%; sensitivity: 79% [95% CI: 58%-95%]; specificity: 78% [95% CI: 65%-88%]). The results broaden the scope of previous studies by incorporating different pathogens, variable levels of disease severity, and different ancestral background of patients, and add confirmatory support to the clinical utility of these 2-transcript biomarkers.
最近,提出了一个由 2 个转录本宿主 RNA 组成的生物标志物特征,用于区分发热儿童的细菌性和病毒性感染。我们在不同的疾病情况下评估了该特征的性能,即一组患有不同感染病因的急性腹泻的墨西哥儿童(n = 174)。我们首先检查了患者的混合背景,表明他们大多数人具有以美洲原住民遗传为主要背景,并有不同程度的欧洲背景(范围从 0%到 57%)。结果证实,RNA 测试可以区分感染的病毒和细菌原因(t 检验;P 值= 6.94×10;AUC= 80%;灵敏度:68%[95%CI:55%-79%];特异性:84%[95%CI:78%-90%]),但信号的强度因病原体的不同而有很大差异,信号更强的是志贺菌(P 值= 3.14×10;AUC= 89;灵敏度:70%[95%CI:57%-83%];特异性:100%[95%CI:100%-100%])。当排除轻度病例时,该测试的准确性显著提高(P 值= 2.13×10;AUC= 85%;灵敏度:79%[95%CI:58%-95%];特异性:78%[95%CI:65%-88%])。这些结果通过纳入不同的病原体、不同的疾病严重程度和不同的患者祖先背景,扩大了先前研究的范围,并为这些 2 个转录本生物标志物的临床实用性提供了确认性支持。