Division of Cardiology, Duke University, Durham, NC
Duke Clinical Research Institute, Duke University, Durham, NC.
J Am Heart Assoc. 2018 May 25;7(11):e008894. doi: 10.1161/JAHA.118.008894.
Intensive care unit (ICU) use for initially stable patients presenting with non-ST-segment-elevation myocardial infarction (NSTEMI) varies widely across hospitals and minimally correlates with severity of illness. We aimed to develop a bedside risk score to assist in identifying high-risk patients with NSTEMI for ICU admission.
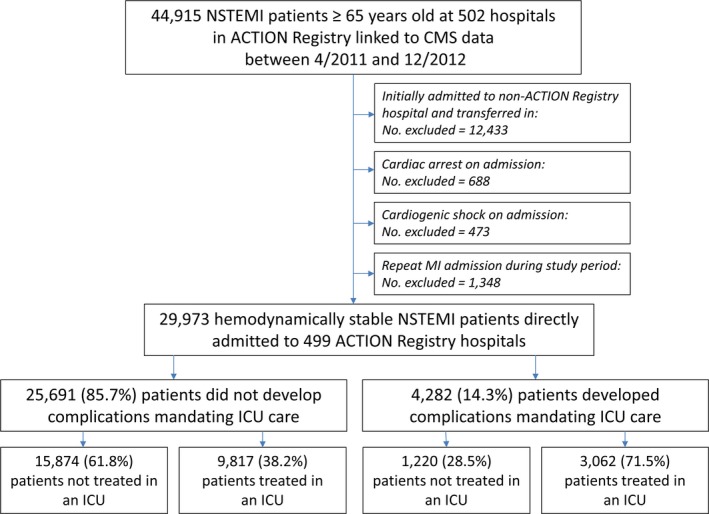
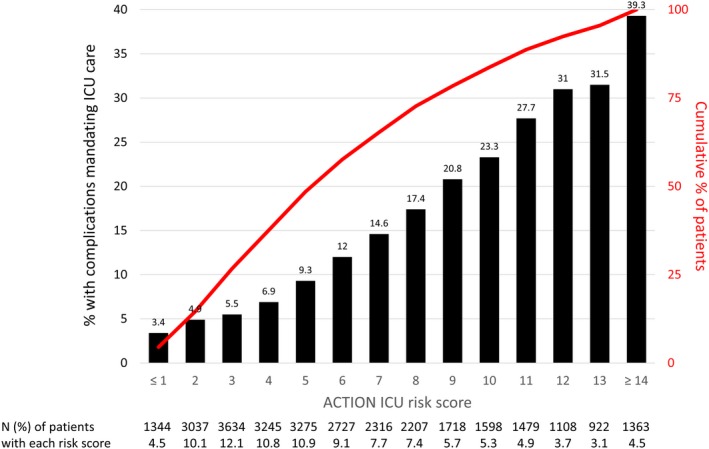
Using the Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Registry linked to Medicare data, we identified patients with NSTEMI aged ≥65 years without cardiogenic shock or cardiac arrest on presentation. Complications requiring ICU care were defined as subsequent development of cardiac arrest, shock, high-grade atrioventricular block, respiratory failure, stroke, or death during the index hospitalization. We developed and validated a model and integer risk score (Acute Coronary Treatment and Intervention Outcomes Network (ACTION) ICU risk score) that uses variables present at hospital admission to predict requirement for ICU care. Of 29 973 patients with NSTEMI, 4282 (14%) developed a complication requiring ICU-level care, yet 12 879 (43%) received care in an ICU. Signs or symptoms of heart failure, initial heart rate, initial systolic blood pressure, initial troponin, initial serum creatinine, prior revascularization, chronic lung disease, ST-segment depression, and age had statistically significant associations with requirement for ICU care after adjusting for other risk factors. The ACTION ICU risk score had a C-statistic of 0.72. It identified 11% of patients as having very high risk (>30%) of developing complications requiring ICU care and 49% as having low likelihood (<10%) of requiring an ICU.
The ACTION ICU risk score quantifies the risk of initially stable patients with NSTEMI developing a complication requiring ICU care, and could be used to more effectively allocate limited ICU resources.
重症监护病房(ICU)对初始稳定的非 ST 段抬高型心肌梗死(NSTEMI)患者的使用在医院之间差异很大,与疾病严重程度的相关性最小。我们旨在开发一种床边风险评分,以帮助识别有 NSTEMI 高危患者需要 ICU 入院。
我们使用急性冠状动脉治疗和干预结果网络(ACTION)注册表与医疗保险数据相关联,确定了年龄≥65 岁且无入院时心源性休克或心脏骤停的 NSTEMI 患者。需要 ICU 护理的并发症定义为随后发展为心脏骤停、休克、高级房室传导阻滞、呼吸衰竭、中风或在索引住院期间死亡。我们开发并验证了一种模型和整数风险评分(急性冠状动脉治疗和干预结果网络(ACTION)ICU 风险评分),该评分使用入院时存在的变量来预测对 ICU 护理的需求。在 29973 例 NSTEMI 患者中,有 4282 例(14%)发生了需要 ICU 级护理的并发症,但有 12879 例(43%)在 ICU 接受了护理。心力衰竭的体征或症状、初始心率、初始收缩压、初始肌钙蛋白、初始血清肌酐、先前的血运重建、慢性肺部疾病、ST 段压低和年龄在调整其他危险因素后与 ICU 护理的需求有统计学显著关联。ACTION ICU 风险评分的 C 统计量为 0.72。它确定了 11%的患者具有极高风险(>30%)发生需要 ICU 护理的并发症,49%的患者发生需要 ICU 护理的可能性较低(<10%)。
ACTION ICU 风险评分量化了初始稳定的 NSTEMI 患者发生需要 ICU 护理的并发症的风险,可用于更有效地分配有限的 ICU 资源。