Zhao Weiwei, Quan Zhiyong, Huang Xufang, Ren Jing, Wen Didi, Zhang Guangwen, Shi Zhongqiang, Yin Hong, Huan Yi
Department of Radiology, Xijing Hospital, Fourth Military Medical University, Xi'an, Shaanxi 710032, P.R. China.
Department of Nuclear Medicine, Xijing Hospital, Fourth Military Medical University, Xi'an, Shaanxi 710032, P.R. China.
Oncol Lett. 2018 Jun;15(6):8349-8356. doi: 10.3892/ol.2018.8384. Epub 2018 Mar 29.
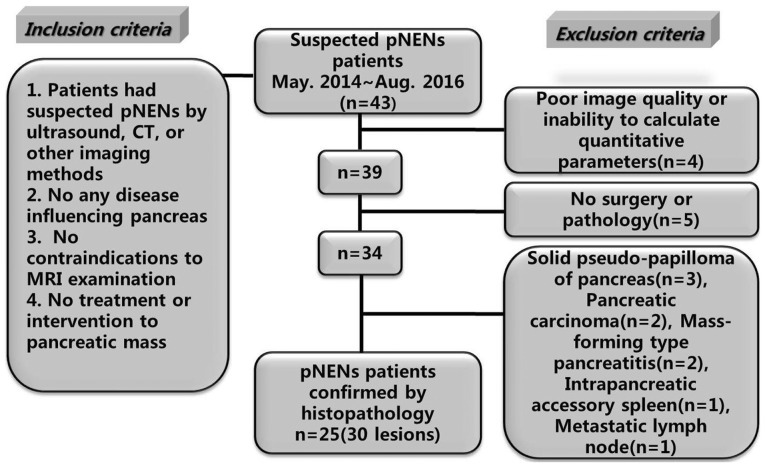
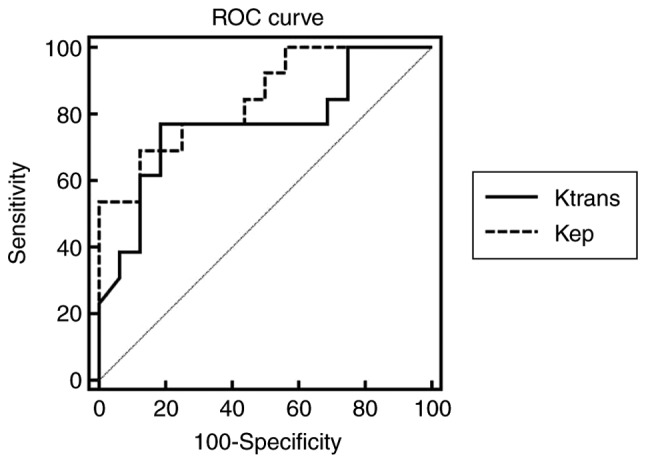
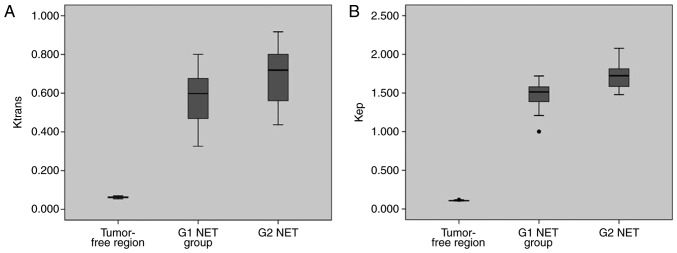
The present study aimed to evaluate the diagnostic efficacy of pharmacokinetic parameters derived from dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) in prospective evaluation of pancreatic neuroendocrine neoplasms (pNENs) grading. A total of 25 histologically proven patients with pNENs (30 lesions in total) who underwent DCE-MRI were enrolled. Lesions were divided into G1, G2 neuroendocrine tumor (NET) and G3 NET/neuroendocrine carcinoma (NEC) groups based on their histological findings according to 2017 World Health Organization Neuroendocrine Tumor Classification Guideline. In addition, the same numbers of tumor-free regions were selected using as normal control group. For each group, pharmacokinetic DCE parameters: volume transfer constant (); contrast transfer rate constant (); extravascular extracellular space volume fraction (v); and plasma volume fraction (v) were calculated with Extended Tofts Linear model. Receiver operator characteristics analysis was conducted to assess the diagnostic efficacy of these parameters in pNENs grading. There were significant differences of , , v and v between tumor-free areas and G1, G2 NET (P<0.001). The and of G1 NET were significantly lower compared with those of G2 ones (P<0.005). The area under the curve of and in differentiating G2 from G1 NET were 0.767 and 0.846, respectively. When was >0.667 and k >1.644, the sensitivity of diagnosing G2 NET was the lowest (53.85%), but the specificity was the highest (93.75%). When was >0.667 or >1.644, the sensitivity of diagnosing G2 NET was 92.31%, but the specificity was 75.00%. Pharmacokinetic parameters of DCE-MRI, particularly the quantitative values of and , are helpful for differentiating G2 NET from G1 ones.
本研究旨在评估动态对比增强磁共振成像(DCE-MRI)得出的药代动力学参数在前瞻性评估胰腺神经内分泌肿瘤(pNENs)分级中的诊断效能。共有25例经组织学证实的pNENs患者(共30个病灶)接受了DCE-MRI检查并被纳入研究。根据2017年世界卫生组织神经内分泌肿瘤分类指南,依据组织学结果将病灶分为G1、G2神经内分泌肿瘤(NET)以及G3 NET/神经内分泌癌(NEC)组。此外,选取相同数量的无肿瘤区域作为正常对照组。对于每组,采用扩展Tofts线性模型计算药代动力学DCE参数:容积转运常数();对比剂转运速率常数();血管外细胞外间隙容积分数(v);以及血浆容积分数(v)。进行受试者操作特征分析以评估这些参数在pNENs分级中的诊断效能。无肿瘤区域与G1、G2 NET之间的、、v和v存在显著差异(P<0.001)。G1 NET的和显著低于G2 NET(P<0.005)。在区分G2与G1 NET时,和的曲线下面积分别为0.767和0.846。当>0.667且k>1.644时,诊断G2 NET的敏感性最低(53.85%),但特异性最高(93.75%)。当>0.667或>1.644时,诊断G2 NET的敏感性为92.31%,但特异性为75.00%。DCE-MRI的药代动力学参数,尤其是和的定量值,有助于区分G2 NET与G1 NET。