Zhao Ming, Guo Li-Li, Huang Ning, Wu Qiong, Zhou Li, Zhao Hui, Zhang Jing, Fu Kuang
Department of MR Diagnosis, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang 150086, P.R. China.
Life Science, GE Healthcare Life Sciences China, Beijing 100176, P.R. China.
Oncol Lett. 2017 Nov;14(5):5418-5426. doi: 10.3892/ol.2017.6895. Epub 2017 Sep 6.
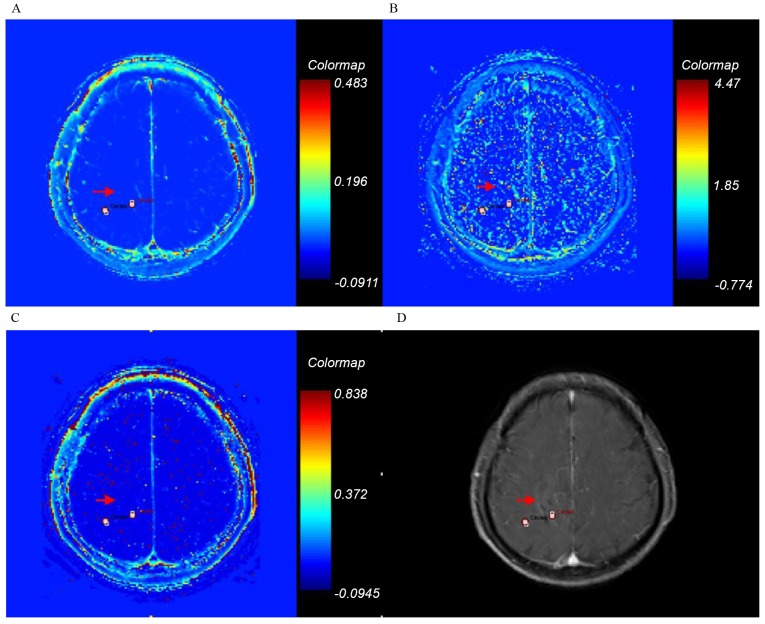
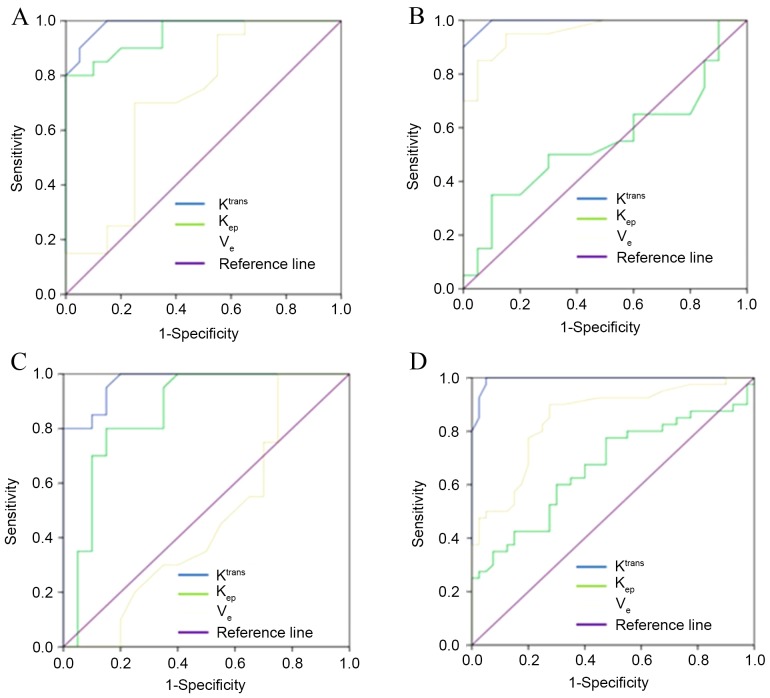
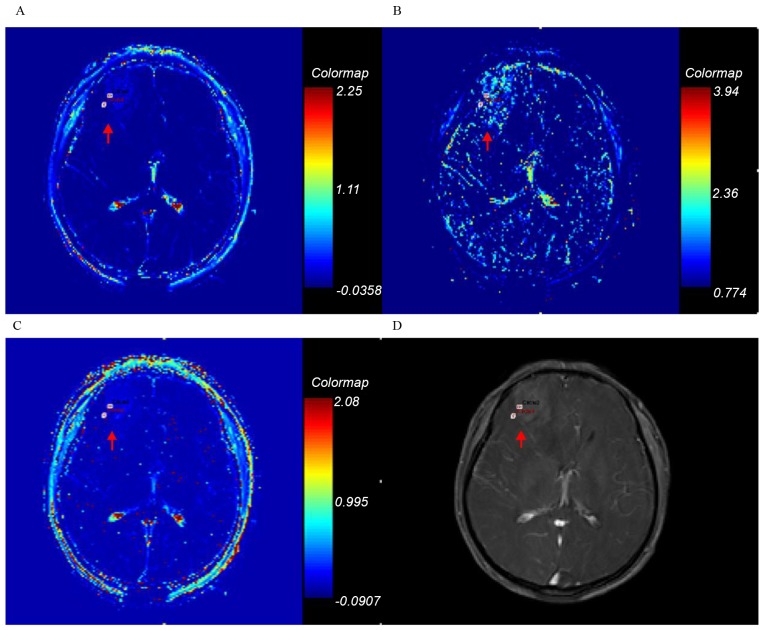
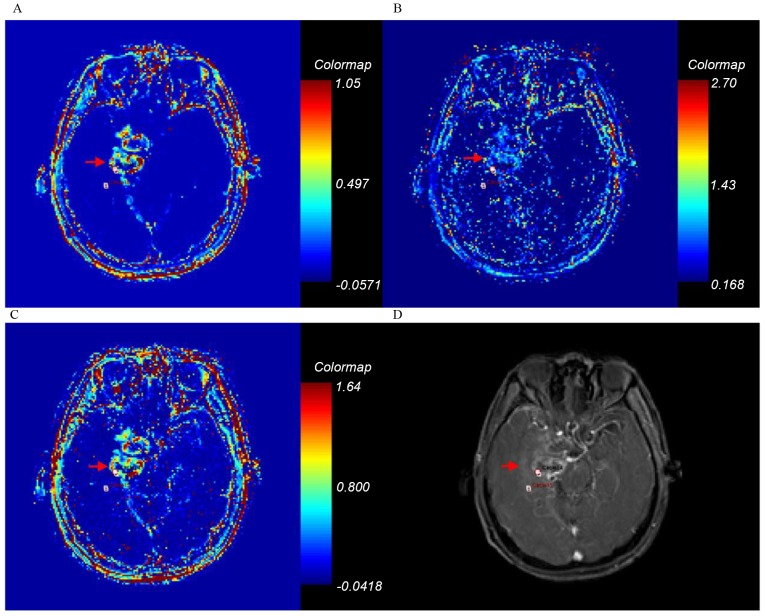
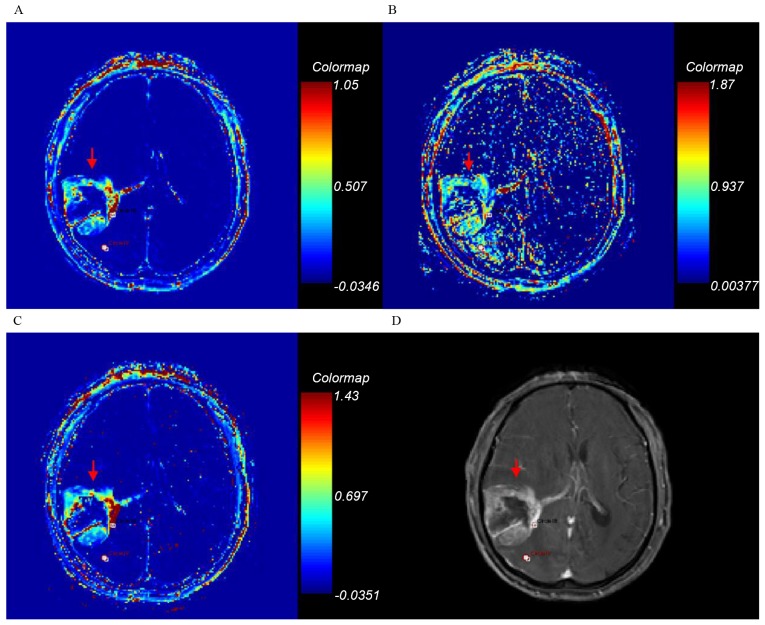
The objective of the present study was to quantitatively analyze the permeability of tumor entity and peritumor edema in glioma grading, using dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI). In the present retrospective study, 80 patients underwent T1-weighted DCE-MRI examination at 3.0 T and the pathological results (including astrocytoma and oligodendroglioma) were obtained between January 2012 and June 2015. All cases were surgically validated as grade I-IV gliomas. The original DCE-MRI data were analyzed using dual compartment modified Tofts model. The forward volume transfer constant (K), backflux rate (k) and fractional volume (v) were calculated with the region of interest selected on the highest permeability area of the tumor entity and peritumor edema. Analysis of variance with the Bonferroni correction was used to compare the values of K, k, and v of the tumor entity and peritumor edema in different glioma grades. The results of the present study revealed that the K, k, and v values in each stage were associated with the pathological grading (r=0.951, 0.804 and 0.766, respectively). There were significant differences identified between different tumor grades in K, k, with the exception being between grades II and III in k. In addition, there was a significant difference revealed between grade I/II and grade III/IV in v. Receiver operator characteristics curve analysis was used to evaluate the diagnosis accuracies of permeability parameters. K was demonstrated to exhibit the highest sensitivity and specificity for evaluating the tumor grade. With the threshold values of 0.160, 0.420 and 0.935 in K on tumor, glioma grades I vs. II, II vs III and III vs. IV may be differentiated with sensitivities of 0.900, 0.950 and 0.950, and specificities of 0.950, 0.950 and 0.850, respectively. Furthermore, associations were observed between the K, k and v values of peritumor edema and the pathological grading in glioma (K r=0.438, P<0.001; K r=0.385, P<0.001; V r=0.397, P<0.001, respectively). K values in peritumoral edema revealed significant differences between low-grade and high-grade glioma. The sensitivity and specificity for K of peritumor edema were 0.975 and 0.950, with a threshold value of 0.007. Therefore, the DCE-MRI parameters of K of tumor entity and peritumor edema in gliomas may be used to accurately differentiate glioma grades.
本研究的目的是使用动态对比增强磁共振成像(DCE-MRI)对神经胶质瘤分级中肿瘤实体和瘤周水肿的通透性进行定量分析。在本回顾性研究中,80例患者于2012年1月至2015年6月期间接受了3.0 T的T1加权DCE-MRI检查,并获得了病理结果(包括星形细胞瘤和少突胶质细胞瘤)。所有病例均经手术验证为I-IV级神经胶质瘤。使用双室改良Tofts模型分析原始DCE-MRI数据。在前瞻性容积转移常数(K)、回流率(k)和容积分数(v)的计算中,感兴趣区域选在肿瘤实体和瘤周水肿的最高通透性区域。采用经Bonferroni校正的方差分析来比较不同神经胶质瘤分级中肿瘤实体和瘤周水肿的K、k和v值。本研究结果显示,各阶段的K、k和v值与病理分级相关(r分别为0.951、0.804和0.766)。不同肿瘤分级之间的K、k存在显著差异,k在II级和III级之间除外。此外,I/II级和III/IV级之间的v存在显著差异。采用受试者工作特征曲线分析来评估通透性参数的诊断准确性。结果表明,K对评估肿瘤分级具有最高的敏感性和特异性。以肿瘤K值的阈值0.160、0.420和0.935,可分别区分I级与II级、II级与III级、III级与IV级神经胶质瘤,敏感性分别为0.900、0.950和0.950,特异性分别为0.950、0.950和0.850。此外,观察到瘤周水肿的K、k和v值与神经胶质瘤的病理分级之间存在相关性(K r = 0.438,P < 0.001;k r = 0.385,P < 0.001;v r = 0.397,P < 0.001)。瘤周水肿的K值在低级别和高级别神经胶质瘤之间存在显著差异。瘤周水肿K值的敏感性和特异性分别为0.975和0.950,阈值为0.007。因此,神经胶质瘤中肿瘤实体和瘤周水肿的DCE-MRI参数K可用于准确区分神经胶质瘤分级。