Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, New York.
Ann Thorac Surg. 2018 Sep;106(3):848-855. doi: 10.1016/j.athoracsur.2018.04.064. Epub 2018 May 26.
The role of postoperative radiotherapy (PORT) in patients with clinical stage III-N2 (cIII-N2) non-small cell lung cancer (NSCLC) treated with induction chemotherapy and surgical resection with persistent ypN2 disease is not well established.
We retrospectively reviewed a prospectively maintained database for patients with cIII-N2 NSCLC who underwent induction chemotherapy followed by resection (2004-2016). Exclusion criteria included induction radiotherapy, non-biopsy-confirmed cN2 disease, incomplete resection, ypN0/1, and nonanatomic resection. The primary outcome was locoregional recurrence (LR); secondary outcomes were disease-free survival (DFS), lung cancer-specific death (LCSD), and overall survival (OS). Associations between variables and outcomes were assessed using Fine and Gray competing risk regression for LR/LCSD and Cox proportional hazard models for survival.
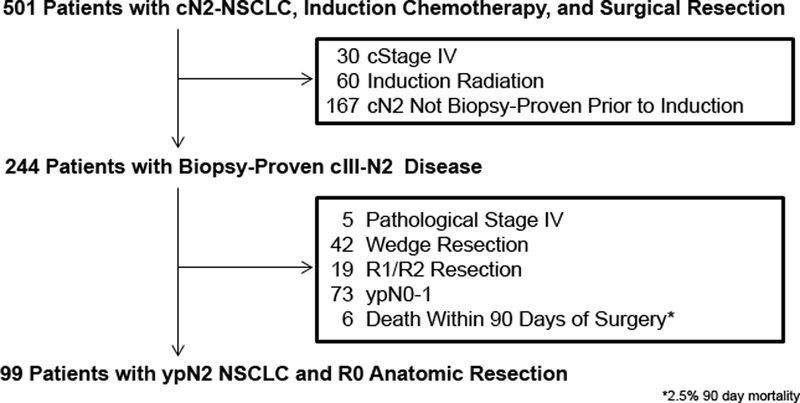
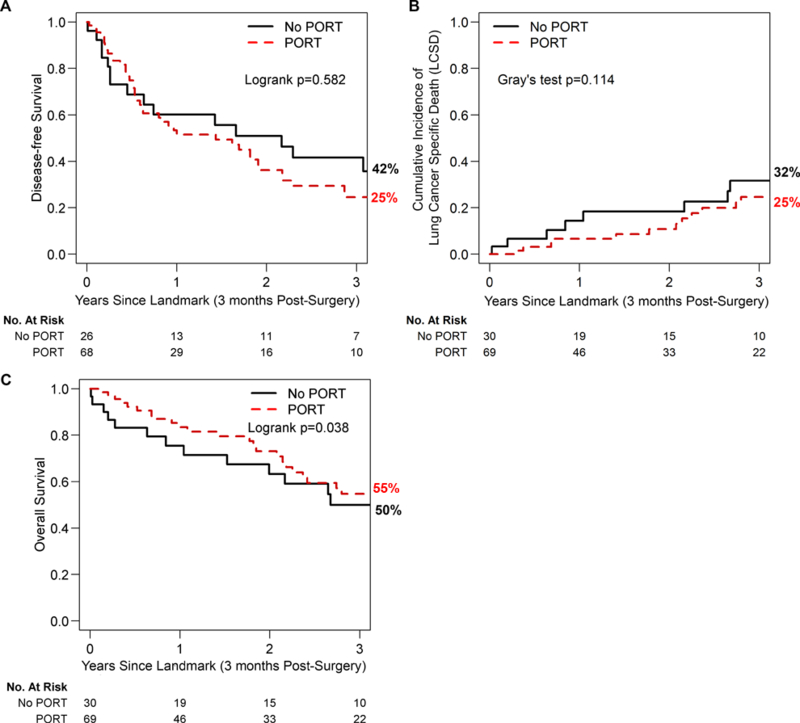
Of the 501 patients identified with cIII-N2 disease, 99 met the inclusion criteria. Median follow-up was 25 months (range, 3-137 months). Sixty-nine patients (70%) received PORT. Sixty (61%) developed a recurrence: 3 (5%) with an initial isolated LR and 57 (95%) with an initial distant recurrence. On multivariable analysis, PORT was not associated with LR (HR, 0.51 [95% CI, 0.22-1.21], p = 0.13). PORT was also not associated with DFS (p = 0.6) or LCSD (p = 0.1). PORT was associated with improved 3-year OS (55% [95% CI, 42%-71%]) versus the no-PORT group (50% [95% CI, 34%-74%]) (p = 0.04).
PORT is not independently associated with decreased LR or improved DFS/LCSD in this patient population. Given that the predominant failure pattern was distant recurrence, future clinical trials should focus on adjuvant systemic therapies, which may decrease distant recurrences in ypN2 patients.
对于接受诱导化疗和手术切除后持续性 ypN2 疾病的临床 III-N2(cIII-N2)非小细胞肺癌(NSCLC)患者,术后放疗(PORT)的作用尚未得到充分确立。
我们回顾性地审查了一个前瞻性维护的数据库,该数据库包含了接受诱导化疗后进行手术切除的 cIII-N2 NSCLC 患者(2004-2016 年)。排除标准包括诱导放疗、非活检证实的 cN2 疾病、不完全切除、ypN0/1 和非解剖性切除。主要结局是局部区域复发(LR);次要结局是无病生存期(DFS)、肺癌特异性死亡(LCSD)和总生存期(OS)。使用 Fine 和 Gray 竞争风险回归分析 LR/LCSD,以及 Cox 比例风险模型分析生存数据,评估变量与结局之间的关系。
在 501 例患有 cIII-N2 疾病的患者中,有 99 例符合纳入标准。中位随访时间为 25 个月(范围,3-137 个月)。69 例(70%)患者接受了 PORT。60 例(61%)患者出现复发:3 例(5%)为初始孤立性 LR,57 例(95%)为初始远处复发。多变量分析显示,PORT 与 LR 无关(HR,0.51 [95%CI,0.22-1.21],p=0.13)。PORT 与 DFS(p=0.6)或 LCSD(p=0.1)也无关。PORT 与 3 年 OS 的提高相关(55% [95%CI,42%-71%]),而无 PORT 组为 50%(95%CI,34%-74%)(p=0.04)。
在该患者人群中,PORT 与降低 LR 或改善 DFS/LCSD 无关。鉴于主要的失败模式是远处复发,未来的临床试验应集中于辅助全身治疗,这可能会降低 ypN2 患者的远处复发率。