Department of Thoracic Surgery and Oncology, The First Affiliated Hospital of Guangzhou Medical University, State Key Laboratory of Respiratory Disease, National Clinical Research Centre for Respiratory Disease, Guangzhou Institute of Respiratory Health, Guangzhou, China.
Department of General Internal Medicine, Sun Yat-sen University Cancer Centre, State Key Laboratory of Oncology in South China, Collaborative Innovation Centre for Cancer Medicine, Guangzhou, China.
BJS Open. 2024 Mar 1;8(2). doi: 10.1093/bjsopen/zrae008.
Stage III non-small cell lung cancer is a heterogeneous disease. Several international guidelines recommend neoadjuvant treatment before surgery; however, upfront surgery is the preferred approach for technically resectable non-small cell lung cancer in East Asia. The aim of this retrospective study was to evaluate the long-term outcomes of curative-intent upfront surgery in stage IIIA/B non-small cell lung cancer.
Patients who underwent curative-intent upfront surgery with stage cIIIA/B non-small cell lung cancer were identified. The clinical and pathological variables and survival outcomes were evaluated.
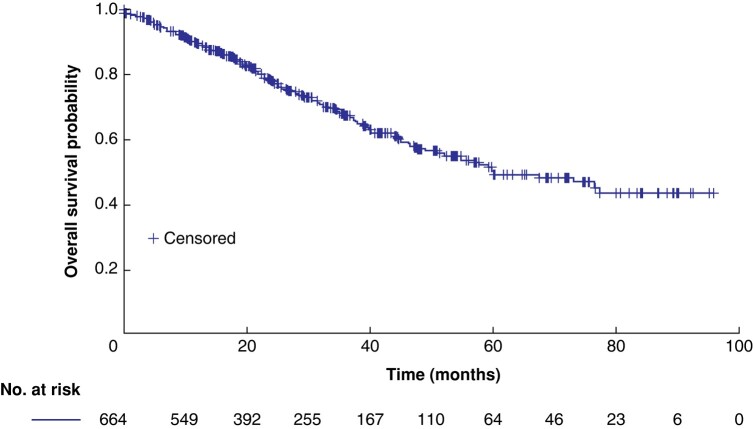
Overall, 664 patients were identified, of whom 320 (48.8%) had N2 disease, 66.7% were males, 49.4% had a smoking history, and 61.2% had lung adenocarcinoma. Lobectomy was the most performed surgical procedure (84.9%). A total of 40 patients (6.02%) had positive margins (R1/R2). The grade III adverse event rate was 2.0% (13 of 664). The median follow-up was 30.6 (range 1.9-97.7) months. At follow-up, the mortality rate was 13.3% (88 of 664) and 37.2% of patients (247 of 664) had recurrence. Lung (101 of 247 (40.9%)) and brain (53 of 247 (21.5%)) were the most common sites of recurrence. The median overall survival was 60.0 (95% c.i. 51.5 to 67.6) months, with overall survival probability at 1, 2, 3, and 5 years being 89.6%, 77.8%, 67.2%, and 49.0% respectively. The R0 cohort showed an improved median overall survival compared with the R1/R2 cohort (67.4 versus 26.5 months respectively; P = greater than 0.001). The multivariable analysis revealed that age greater than or equal to 65 years (HR 1.51, 95% c.i. 1.08 to 2.12; reference = age less than 65 years), tumour size (greater than or equal to 5 cm (HR 2.13, 95% c.i. 1.41 to 3.21) and greater than or equal to 3 cm but less than 5 cm (HR 1.15, 95% c.i. 0.78 to 1.71); reference = less than 3 cm), and adjuvant treatment (chemotherapy (HR 0.69, 95% c.i. 0.49 to 0.96) and targeted therapy (HR 0.30, 95% c.i. 0.12 to 0.76); reference = none) significantly predicted overall survival.
Upfront surgery is an option for the management of stage IIIA/B non-small cell lung cancer.
III 期非小细胞肺癌是一种异质性疾病。几项国际指南建议在手术前进行新辅助治疗;然而,对于东亚有技术可切除的非小细胞肺癌,首选的方法是直接手术。本回顾性研究旨在评估 IIIA/B 期非小细胞肺癌患者根治性直接手术的长期结果。
确定了接受根治性直接手术治疗的 cIIIA/B 期非小细胞肺癌患者。评估了临床和病理变量以及生存结果。
共确定了 664 例患者,其中 320 例(48.8%)有 N2 疾病,66.7%为男性,49.4%有吸烟史,61.2%为肺腺癌。肺叶切除术是最常进行的手术(84.9%)。共有 40 例(6.02%)有阳性切缘(R1/R2)。III 级不良事件发生率为 2.0%(664 例中的 13 例)。中位随访时间为 30.6(范围 1.9-97.7)个月。随访时,死亡率为 13.3%(664 例中的 88 例),37.2%的患者(664 例中的 247 例)复发。肺部(247 例中的 101 例(40.9%))和脑部(247 例中的 53 例(21.5%))是最常见的复发部位。中位总生存期为 60.0(95%置信区间 51.5 至 67.6)个月,1、2、3 和 5 年的总生存率分别为 89.6%、77.8%、67.2%和 49.0%。R0 队列的中位总生存期优于 R1/R2 队列(分别为 67.4 个月和 26.5 个月;P 大于 0.001)。多变量分析显示,年龄大于或等于 65 岁(HR 1.51,95%置信区间 1.08 至 2.12;参考年龄小于 65 岁)、肿瘤大小(大于或等于 5cm(HR 2.13,95%置信区间 1.41 至 3.21)和大于或等于 3cm 但小于 5cm(HR 1.15,95%置信区间 0.78 至 1.71);参考小于 3cm)和辅助治疗(化疗(HR 0.69,95%置信区间 0.49 至 0.96)和靶向治疗(HR 0.30,95%置信区间 0.12 至 0.76);参考无)显著预测总生存期。
直接手术是治疗 IIIA/B 期非小细胞肺癌的一种选择。