Cardiovascular Outcomes Research, University of Missouri-Kansas City, Saint-Luke's Mid-America Heart Institute, Kansas City, Missouri.
Division of Cardiology, Washington University School of Medicine in Saint Louis, Barnes-Jewish Hospital, Saint Louis, Missouri.
JACC Heart Fail. 2018 Jun;6(6):465-473. doi: 10.1016/j.jchf.2018.02.002.
This study sought to describe the health status of outpatients with heart failure and reduced ejection fraction (HFrEF) by sex, race/ethnicity, and socioeconomic status (SES).
Although a primary goal in treating patients with HFrEF is to optimize health status, whether disparities by sex, race/ethnicity, and SES exist is unknown.
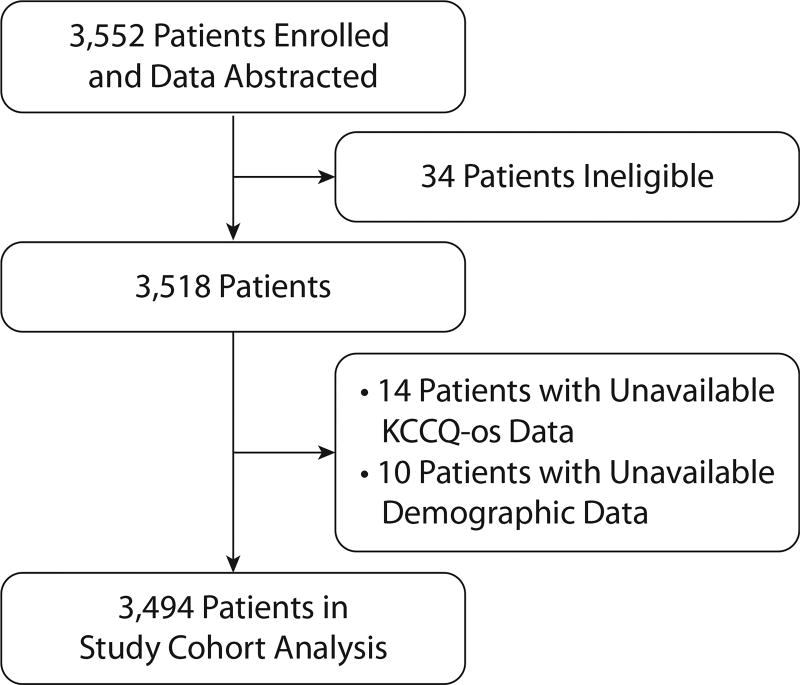
In the CHAMP-HF (Change the Management of Patients with Heart Failure) registry, the associations among sex, race, and SES and health status, as measured by the Kansas City Cardiomyopathy Questionnaire-overall summary (KCCQ-os) score (range 0 to 100; higher scores indicate better health status) was compared among 3,494 patients from 140 U.S. clinics. SES was categorized by total household income. Hierarchical multivariate linear regression estimated differences in KCCQ-os score after adjusting for 31 patient characteristics and 10 medications.
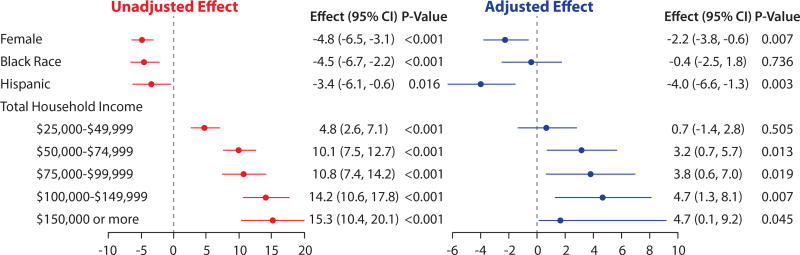
Overall mean KCCQ-os scores were 64.2 ± 24.0 but lower for women (29% of sample; 60.3 ± 24.0 vs. 65.9 ± 24.0, respectively; p < 0.001), for blacks (60.5 ± 25.0 vs. 64.9 ± 23.0, respectively; p < 0.001), for Hispanics (59.1 ± 21.0 vs. 64.9 ± 23.0, respectively; p < 0.001), and for those with the lowest income (<$25,000; mean: 57.1 vs. 63.1 to 74.7 for other income categories; p < 0.001). Fully adjusted KCCQ-os scores were 2.2 points lower for women (95% confidence interval [CI]: -3.8 to -0.6; p = 0.007), no different for blacks (p = 0.74), 4.0 points lower for Hispanics (95% CI: -6.6 to -1.3; p = 0.003), and lowest in the poorest patients (4.7 points lower than those with the highest income (95% CI: 0.1 to 9.2; p = 0.045; p for trend = 0.003).
Among outpatients with HFrEF, women, blacks, Hispanics, and poorer patients had worse health status, which remained significant for women, Hispanics, and poorer patients in fully adjusted analyses. This suggests an opportunity to further optimize treatment to reduce these observed disparities.
本研究旨在按性别、种族和社会经济地位(SES)描述射血分数降低的心力衰竭(HFrEF)门诊患者的健康状况。
尽管治疗 HFrEF 患者的主要目标是优化健康状况,但尚不清楚是否存在性别、种族和 SES 差异。
在 CHAMP-HF(改变心力衰竭患者管理)登记研究中,通过堪萨斯城心肌病问卷整体摘要(KCCQ-os)评分(范围 0 至 100;评分越高表示健康状况越好)比较了来自美国 140 家诊所的 3494 名患者的性别、种族和 SES 与健康状况之间的关联。SES 按家庭总收入进行分类。分层多变量线性回归估计了调整 31 项患者特征和 10 种药物后 KCCQ-os 评分的差异。
总体平均 KCCQ-os 评分为 64.2 ± 24.0,但女性较低(样本的 29%;分别为 60.3 ± 24.0 和 65.9 ± 24.0;p < 0.001),黑人较低(分别为 60.5 ± 25.0 和 64.9 ± 23.0;p < 0.001),西班牙裔较低(分别为 59.1 ± 21.0 和 64.9 ± 23.0;p < 0.001),收入最低的患者较低(<$25,000;均值:57.1 比其他收入类别低 63.1 至 74.7;p < 0.001)。女性的完全调整 KCCQ-os 评分低 2.2 分(95%置信区间[CI]:-3.8 至-0.6;p = 0.007),黑人无差异(p = 0.74),西班牙裔低 4.0 分(95%CI:-6.6 至-1.3;p = 0.003),最贫困患者最低(比收入最高的患者低 4.7 分(95%CI:0.1 至 9.2;p = 0.045;p 趋势= 0.003)。
在 HFrEF 门诊患者中,女性、黑人、西班牙裔和贫困患者的健康状况较差,在完全调整分析中,女性、西班牙裔和贫困患者的健康状况仍存在显著差异。这表明有机会进一步优化治疗以减少这些观察到的差异。