Department of Gastroenterology, Hepatobiliary and Pancreatic Medical Oncology Division, Kanagawa Cancer Center, Yokohama, Japan.
Department of Gastroenterology, Kanazawa University Hospital, Ishikawa, Japan.
Cancer Sci. 2018 Aug;109(8):2549-2557. doi: 10.1111/cas.13656. Epub 2018 Jun 27.
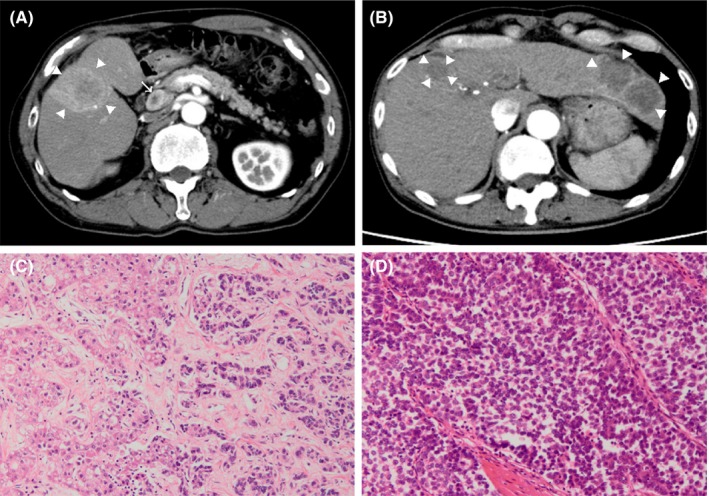
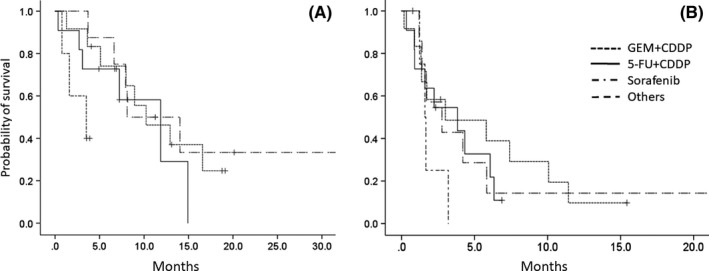
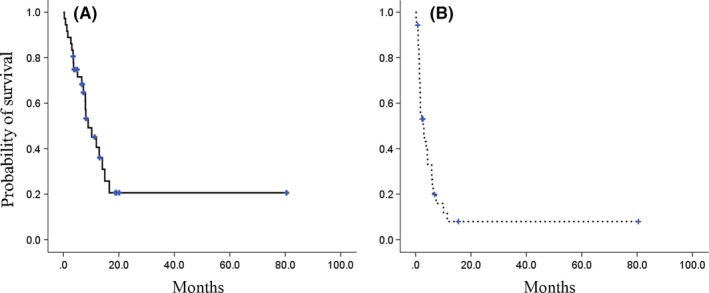
We conducted a multicenter retrospective analysis to evaluate the efficacy of systemic chemotherapy for unresectable combined hepatocellular and cholangiocarcinoma. We enrolled 36 patients with pathologically proven, unresectable combined hepatocellular and cholangiocarcinoma treated with systemic chemotherapy. The log-rank test determined the significance of each prognostic factor. Elevated alpha-fetoprotein, carcinoembryonic antigen and carbohydrate antigen 19-9 levels were observed in 58.3%, 16.7% and 38.9% of patients, respectively. First-line chemotherapy included platinum-containing regimens consisting of gemcitabine/cisplatin (n = 12) and fluorouracil/cisplatin (n = 11), sorafenib (n = 5) and others (n = 8). The median overall and progression-free survival times were 8.9 and 2.8 months, respectively, with an overall response rate of 5.6%. Prognostic factors associated with negative outcomes included poor performance status, no prior primary tumor resection, a Child-Pugh class of B, and elevated carcinoembryonic antigen levels with a hazard ratio of 2.25, 2.48, 3.25 and 2.84 by univariate analysis, respectively. The median overall survival times of the gemcitabine/cisplatin, fluorouracil/cisplatin, sorafenib and other groups were 11.9, 10.2, 3.5 and 8.1 months, respectively. Multivariate analysis revealed that the overall survival of patients within the sorafenib monotherapy group was poor compared with platinum-containing regimens (HR: 15.83 [95% CI: 2.25-111.43], P = .006). All 7 patients in the sorafenib group had progressive disease, including 2 patients with second-line therapy. In conclusion, the platinum-containing regimens such as gemcitabine/cisplatin were associated with more favorable outcomes than sorafenib monotherapy for unresectable combined hepatocellular and cholangiocarcinoma.
我们进行了一项多中心回顾性分析,以评估不可切除的肝细胞癌和胆管细胞癌的全身化疗疗效。我们纳入了 36 例经病理证实、不可切除的肝细胞癌和胆管细胞癌患者,这些患者接受了全身化疗。对数秩检验确定了每个预后因素的意义。58.3%、16.7%和 38.9%的患者分别出现了甲胎蛋白、癌胚抗原和糖类抗原 19-9 水平升高。一线化疗包括含铂方案(吉西他滨/顺铂,n=12;氟尿嘧啶/顺铂,n=11)、索拉非尼(n=5)和其他方案(n=8)。中位总生存期和无进展生存期分别为 8.9 和 2.8 个月,总缓解率为 5.6%。与不良结局相关的预后因素包括一般状况差、无原发性肿瘤切除术史、Child-Pugh 分级为 B 级以及癌胚抗原水平升高,单因素分析的危险比分别为 2.25、2.48、3.25 和 2.84。吉西他滨/顺铂、氟尿嘧啶/顺铂、索拉非尼和其他组的中位总生存时间分别为 11.9、10.2、3.5 和 8.1 个月。多因素分析显示,索拉非尼单药组患者的总生存情况较差,与含铂方案相比(HR:15.83[95%CI:2.25-111.43],P=0.006)。索拉非尼组的 7 例患者均发生进展性疾病,其中 2 例接受二线治疗。总之,对于不可切除的肝细胞癌和胆管细胞癌,含铂方案(如吉西他滨/顺铂)的疗效优于索拉非尼单药治疗。