Wong Kerry L M, Radovich Emma, Owolabi Onikepe O, Campbell Oona M R, Brady Oliver J, Lynch Caroline A, Benova Lenka
Department of Infectious Disease Epidemiology, Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, Keppel Street, London, WC1E 7HT, UK.
Guttmacher Institute, 125 Maiden Lane 7th Floor, New York, NY, 10038, USA.
BMC Health Serv Res. 2018 Jun 1;18(1):397. doi: 10.1186/s12913-018-3225-4.
In Nigeria, the provision of public and private healthcare vary geographically, contributing to variations in one's healthcare surroundings across space. Facility-based delivery (FBD) is also spatially heterogeneous. Levels of FBD and private FBD are significantly lower for women in certain south-eastern and northern regions. The potential influence of childbirth services frequented by the community on individual's barriers to healthcare utilization is under-studied, possibly due to the lack of suitable data. Using individual-level data, we present a novel analytical approach to examine the relationship between women's reasons for homebirth and community-level, health-seeking surroundings. We aim to assess the extent to which cost or finance acts as a barrier for FBD across geographic areas with varying levels of private FBD in Nigeria.
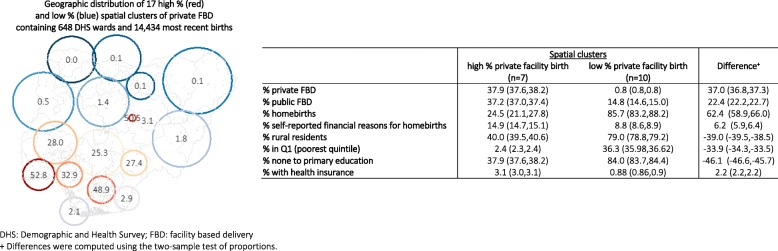
The most recent live births of 20,467 women were georeferenced to 889 locations in the 2013 Nigeria Demographic and Health Survey. Using these locations as the analytical unit, spatial clusters of high/low private FBD were detected with Kulldorff statistics in the SatScan software package. We then obtained the predicted percentages of women who self-reported financial reasons for homebirth from an adjusted generalized linear model for these clusters.
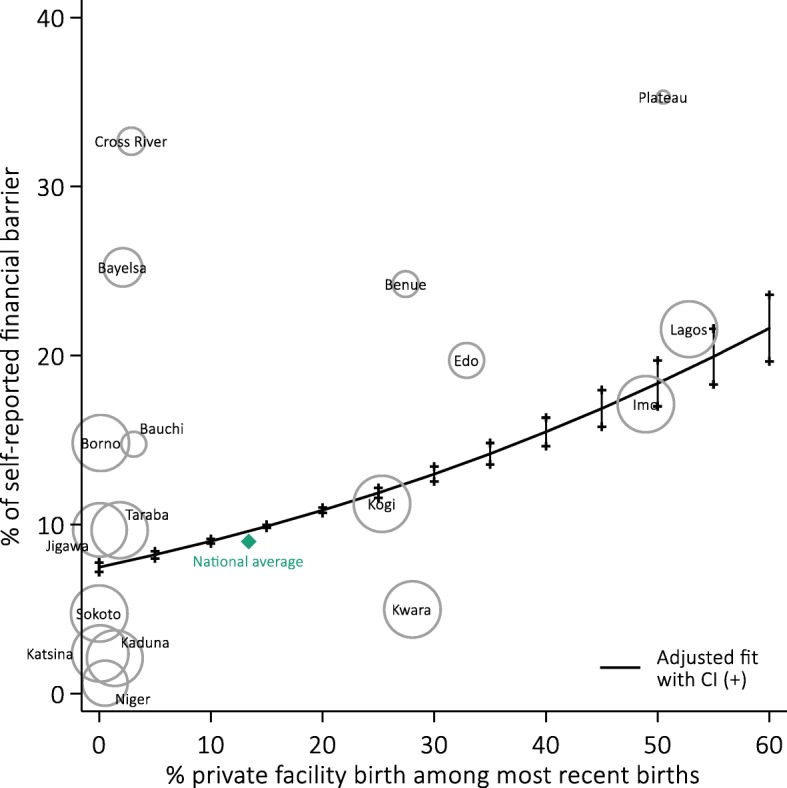
Overall private FBD was 13.6% (95%CI = 11.9,15.5). We found ten clusters of low private FBD (average level: 0.8, 95%CI = 0.8,0.8) and seven clusters of high private FBD (average level: 37.9, 95%CI = 37.6,38.2). Clusters of low private FBD were primarily located in the north, and the Bayelsa and Cross River States. Financial barrier was associated with high private FBD at the cluster level - 10% increase in private FBD was associated with + 1.94% (95%CI = 1.69,2.18) in nonusers citing cost as a reason for homebirth.
In communities where private FBD is common, women who stay home for childbirth might have mild increased difficulties in gaining effective access to public care, or face an overriding preference to use private services, among other potential factors. The analytical approach presented in this study enables further research of the differentials in individuals' reasons for service non-uptake across varying contexts of healthcare surroundings. This will help better devise context-specific strategies to improve health service utilization in resource-scarce settings.
在尼日利亚,公共和私人医疗保健的提供在地理上存在差异,导致人们在不同空间的医疗环境有所不同。基于设施的分娩(FBD)在空间上也存在异质性。在东南部和北部的某些地区,女性的FBD水平和私人FBD水平显著较低。社区中常见的分娩服务对个人利用医疗保健的障碍的潜在影响研究不足,这可能是由于缺乏合适的数据。我们使用个体层面的数据,提出一种新颖的分析方法来研究女性在家分娩的原因与社区层面的就医环境之间的关系。我们旨在评估在尼日利亚私人FBD水平不同的地理区域中,成本或资金在多大程度上成为FBD的障碍。
在2013年尼日利亚人口与健康调查中,将20467名妇女最近的活产记录地理定位到889个地点。以这些地点作为分析单位,使用SatScan软件包中的Kulldorff统计量检测高/低私人FBD的空间聚类。然后,我们从针对这些聚类的调整后的广义线性模型中获得了自我报告因经济原因在家分娩的妇女的预测百分比。
总体私人FBD为13.6%(95%CI = 11.9,15.5)。我们发现了10个低私人FBD聚类(平均水平:0.8,95%CI = 0.8,0.8)和7个高私人FBD聚类(平均水平:37.9,95%CI = 37.6,38.2)。低私人FBD聚类主要位于北部以及巴耶尔萨州和克罗斯河州。在聚类层面,经济障碍与高私人FBD相关——私人FBD每增加10%,将导致将成本作为在家分娩原因的未使用者增加1.94%(95%CI =1.69,2.18)。
在私人FBD普遍存在的社区中,在家分娩的妇女在有效获得公共医疗服务方面可能会遇到略有增加的困难,或者在其他潜在因素中,面临使用私人服务的压倒性偏好。本研究中提出的分析方法能够进一步研究在不同医疗环境背景下个人不使用服务的原因差异。这将有助于更好地制定针对具体情况的策略,以提高资源稀缺地区的医疗服务利用率。