Amin Saloni, Shah Samidh, Desai Mira, Shah Asha, Maheriya K M
Department of Pharmacology, B. J. Medical College, Ahmedabad, Gujarat, India.
Department of Medicine, B. J. Medical College, Ahmedabad, Gujarat, India.
Perspect Clin Res. 2018 Apr-Jun;9(2):70-75. doi: 10.4103/picr.PICR_64_17.
To analyze clinical spectrum, seriousness, outcome, causality, severity and preventability of ADRs in geriatrics and pediatric patients.
All ADRs reported in geriatrics (≥ 65 years) and pediatrics (≤ 12 years) indoor as well outdoor patients from January, 2010 to April, 2016 at ADR monitoring centre, Department of Pharmacology, B. J. Medical College and Civil Hospital were identified. A retrospective analysis was carried out for clinical presentation, causality (as per WHO-UMC scale and Naranjo's algorithm), severity (Hatwig and Seigel scale) and preventability (Schaumock and Thornton criteria).
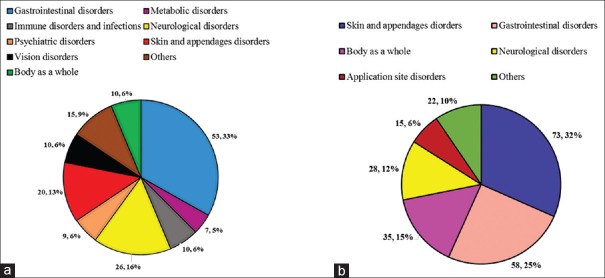
Out of 3690 ADRs, 160 were in geriatric patients (4.33%) while 231 in pediatric patients (6.26%). The most commonly affected body system was gastrointestinal (53, 33.13%) followed by neurological disorders (26, 16.25%) in geriatric patients. While in pediatric patients, the most commonly affected body system was skin and appendages (73, 31.60 %) followed by gastrointestinal disorders (58, 25.11%). The most common causal drugs in geriatric patients was cardiovascular (38, 23.75%) followed by antimicrobials (28, 13.25%). While in pediatric patients, the most common causal drug group was antimicrobials (85, 33.46%) followed by blood products (36, 14.12%). Total 17 ADRs reported following vaccination, 7 (41.17%) were injection site abscess and 11 (64.70%) were due to pentavalent vaccine. Polypharmacy was common in geriatrics (31, 19.37%). Causality assessment for majority of ADRs in geriatrics (83, 52.5%) and pediatrics (171, 67.32%) were probable.
ADRs are common in geriatric and pediatric patients usually within four weeks of oral therapy. Active surveillance of drug safety monitoring in these vulnerable population is recommended.
分析老年患者和儿科患者药物不良反应(ADR)的临床谱、严重程度、转归、因果关系、严重性及可预防性。
确定2010年1月至2016年4月在BJ医学院药理系和市民医院ADR监测中心报告的老年(≥65岁)和儿科(≤12岁)住院及门诊患者的所有ADR。对临床表现、因果关系(按照WHO-UMC量表和Naranjo算法)、严重程度(Hatwig和Seigel量表)及可预防性(Schaumock和Thornton标准)进行回顾性分析。
在3690例ADR中,老年患者有160例(4.33%),儿科患者有231例(6.26%)。老年患者中最常受累的身体系统是胃肠道(53例,33.13%),其次是神经系统疾病(26例,16.25%)。而在儿科患者中,最常受累的身体系统是皮肤及附属器(73例,31.60%),其次是胃肠道疾病(58例,25.11%)。老年患者中最常见的因果药物是心血管药物(38例,23.75%),其次是抗菌药物(28例,13.25%)。而在儿科患者中,最常见的因果药物组是抗菌药物(85例,33.46%),其次是血液制品(36例,14.12%)。共报告17例接种疫苗后的ADR,7例(41.17%)为注射部位脓肿,11例(64.70%)与五价疫苗有关。老年患者中多重用药情况常见(31例,19.37%)。老年患者(83例,52.5%)和儿科患者(171例,67.32%)中大多数ADR的因果关系评估为可能。
ADR在老年患者和儿科患者中常见,通常发生在口服治疗的四周内。建议对这些弱势群体进行药物安全性监测的主动监测。