Modi Anal, Desai Mira, Shah Samidh, Shah Bela
Department of Pharmacology, B. J. Medical College, Ahmedabad, Gujarat, India.
Department of Skin and VD, B. J. Medical College, Ahmedabad, Gujarat, India.
Indian J Dermatol. 2019 May-Jun;64(3):250. doi: 10.4103/ijd.IJD_682_16.
Skin is one of the major target organ for adverse drug reactions (ADRs). The incidence of dermatological ADRs among indoor patients in developed countries ranges from 1-3%, whereas in developing countries such as India, it is 2-5%.
To analyze the clinical spectrum, seriousness, outcome, causality, severity, and preventability of the cutaneous ADRs.
All cutaneous ADRs reported at the Regional Adverse Drug Reaction Monitoring Center between January 2013 to May 2016 were identified and evaluated. A retrospective analysis was carried out for clinical presentation, causality (as per the WHO-UMC scale and the Naranjo'a reactions (ADRs) Severity (Hartwig and Seigel scale), and preventability (Schumock and Thornton criteria) of a said drug.
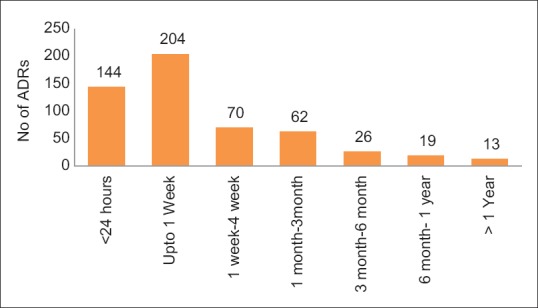
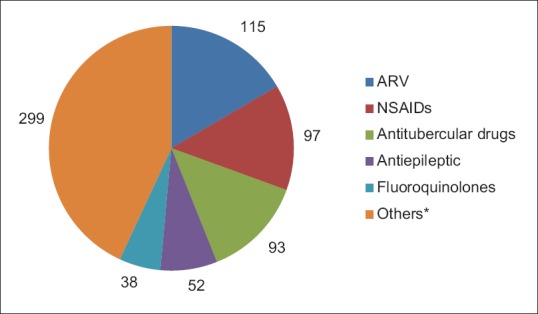
Out of 2171 ADRs reported during study period, 538 were cutaneous ADRs (24.78%). The most common clinical presentation was maculopapular rash (58.92%) followed by itching (10.59%), and Stevens-Johnson syndrome (4.83%). The time relationship of cutaneous ADRs to drug therapy revealed that they can develop within 1 week to 1 year of treatment. Most common causal drug groups were antimicrobials (46%), non-steroidal anti-inflammatory drugs (NSAIDs) (18%), and antiepileptics (10%). Polypharmacy was observed in 7% of the cases. Most of the cutaneous ADRs were non-serious (91%), however, 10 were life-threatening and 1 was resulted in death due to the Stevens-Johnson syndrome. Causality category for majority of cutaneous ADRs was possible. Although majority of cutaneous ADRs were moderately severe (81%), however, not preventable (89%).
The occurrence of cutaneous ADRs is common and they developed within 1 week of therapy. Antimicrobial agents and NSAIDs are the most common implicated drug class. Hence, physicians should closely monitor the patient in the first week while using such therapy for early detection and prevention of cutaneous ADRs.
皮肤是药物不良反应(ADR)的主要靶器官之一。发达国家住院患者中皮肤ADR的发生率为1%-3%,而在印度等发展中国家,这一比例为2%-5%。
分析皮肤ADR的临床谱、严重程度、转归、因果关系、严重性及可预防性。
确定并评估2013年1月至2016年5月期间区域药物不良反应监测中心报告的所有皮肤ADR。对所述药物的临床表现、因果关系(根据世界卫生组织药物不良反应监测中心量表和纳兰霍量表)、严重程度(哈特维希和西格尔量表)及可预防性(舒莫克和桑顿标准)进行回顾性分析。
在研究期间报告的2171例ADR中,538例为皮肤ADR(24.78%)。最常见的临床表现为斑丘疹(58.92%),其次是瘙痒(10.59%)和史蒂文斯-约翰逊综合征(4.83%)。皮肤ADR与药物治疗的时间关系显示,它们可在治疗的1周内至1年内出现。最常见的致病药物类别为抗菌药物(46%)、非甾体抗炎药(NSAIDs)(18%)和抗癫痫药(10%)。7%的病例存在联合用药情况。大多数皮肤ADR不严重(91%),然而,有10例危及生命,1例因史蒂文斯-约翰逊综合征死亡。大多数皮肤ADR的因果关系类别为“可能”。虽然大多数皮肤ADR为中度严重(81%),但不可预防(89%)。
皮肤ADR很常见,且在治疗1周内出现。抗菌药物和NSAIDs是最常见的致病药物类别。因此,医生在使用此类药物治疗时应在第一周密切监测患者,以便早期发现和预防皮肤ADR。