Altmann Uwe, Thielemann Désirée, Zimmermann Anna, Steffanowski Andrés, Bruckmeier Ellen, Pfaffinger Irmgard, Fembacher Andrea, Strauß Bernhard
Institute of Psychosocial Medicine and Psychotherapy, Universitätsklinikum Jena, Jena, Germany.
Faculty of Applied Psychology, SRH University Heidelberg, Heidelberg, Germany.
Front Psychol. 2018 May 16;9:748. doi: 10.3389/fpsyg.2018.00748. eCollection 2018.
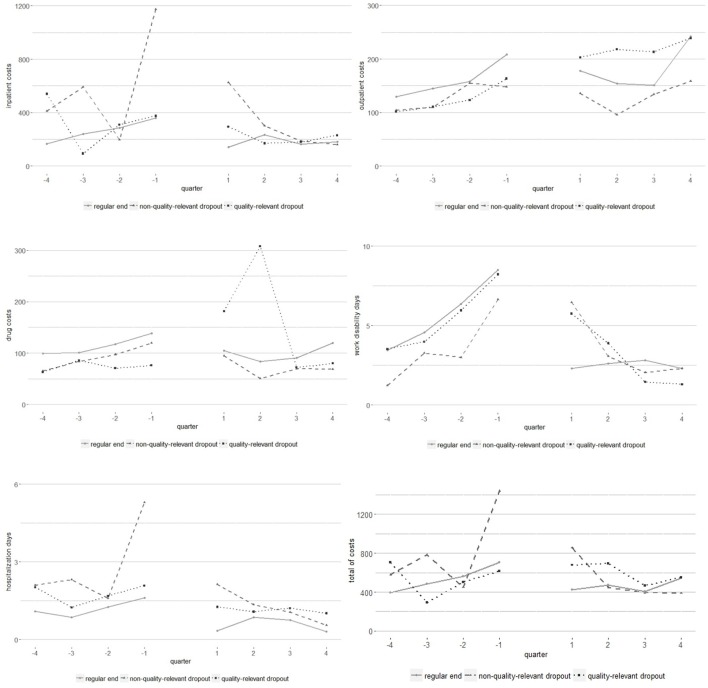
In view of a shortage of health care costs, monetary aspects of psychotherapy become increasingly relevant. The present study examined the pre-post reduction of impairment and direct health care costs depending on therapy termination (regularly terminated, dropout with an unproblematic reason, and dropout with a quality-relevant reason) and the association of symptom and cost reduction. In a naturalistic longitudinal study, we examined a disorder heterogeneous sample of = 584 outpatients who were either treated with cognitive-behavioral, psychodynamic, or psychoanalytic therapy. Depression, anxiety, stress, and somatization were assessed with the Patient Health Questionnaire (PHQ). Annual amounts of inpatient costs, outpatient costs, medication costs, days of hospitalization, work disability days, utilization of psychotherapy, and utilization of pharmacotherapy 1 year before therapy and 1 year after therapy were provided by health care insurances. Symptom and cost reduction were analyzed using -tests. Associations between symptom and cost reduction were examined using partial correlations and hierarchical linear models. Patients who terminated therapy regularly showed the largest symptom reduction ( = 0.981-1.22). Patients who dropped out due to an unproblematic reason and patients who terminated early due to a quality-relevant reason showed significant but small effects of symptom reductions (e.g., depression: = 0.429 vs. = 0.366). For patients with a regular end and those dropping out due to a quality-relevant reason, we observed a significant reduction of work disability (diff in % of pre-test value = 56.3 vs. 42.9%) and hospitalization days (52.8 vs. 35.0%). Annual inpatient costs decreased in the group with a regular therapy end (31.5%). Furthermore, reduction of symptoms on the one side and reduction of work disability days and psychotherapy utilization on the other side were significant correlated ( = 0.091-0.135). Health care costs and symptoms were reduced in each of the three groups. The average symptom and cost reduction of patients with a quality-relevant dropout suggested that not each dropout might be seen as therapy failure.
鉴于医疗保健成本短缺,心理治疗的货币方面变得越来越重要。本研究考察了根据治疗终止情况(正常终止、因无问题原因退出和因质量相关原因退出)导致的损伤和直接医疗保健成本的前后降低情况,以及症状减轻与成本降低之间的关联。在一项自然主义纵向研究中,我们考察了一个由584名门诊患者组成的异质性疾病样本,这些患者接受了认知行为疗法、心理动力疗法或精神分析疗法。使用患者健康问卷(PHQ)评估抑郁、焦虑、压力和躯体化情况。医疗保险提供了治疗前1年和治疗后1年的住院费用、门诊费用、药物费用、住院天数、工作残疾天数、心理治疗利用率和药物治疗利用率的年度金额。使用t检验分析症状和成本降低情况。使用偏相关和分层线性模型检验症状减轻与成本降低之间的关联。正常终止治疗的患者症状减轻幅度最大(t = 0.981 - 1.22)。因无问题原因退出的患者和因质量相关原因提前终止治疗的患者症状减轻有显著但较小的效果(例如,抑郁:t = 0.429对t = 0.366)。对于正常结束治疗的患者和因质量相关原因退出的患者,我们观察到工作残疾(预测试值百分比差异 = 56.3对42.9%)和住院天数(52.8对35.0)有显著减少。正常治疗结束组的年度住院费用下降(31.5%)。此外,一方面症状减轻与另一方面工作残疾天数减少和心理治疗利用率减少之间存在显著相关性(r = 0.091 - 0.135)。三组患者的医疗保健成本和症状均有所降低。因质量相关原因退出治疗的患者的平均症状和成本降低表明,并非每次退出都可被视为治疗失败。