Doman Sydney E, Girish Akanksha, Nemeth Christina L, Drummond Gabrielle T, Carr Patrice, Garcia Maxine S, Johnston Michael V, Kannan Sujatha, Fatemi Ali, Zhang Jiangyang, Wilson Mary Ann
Hugo W. Moser Research Institute at Kennedy Krieger, Baltimore, MD, United States.
Department of Neurology, The Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Front Neurol. 2018 May 8;9:304. doi: 10.3389/fneur.2018.00304. eCollection 2018.
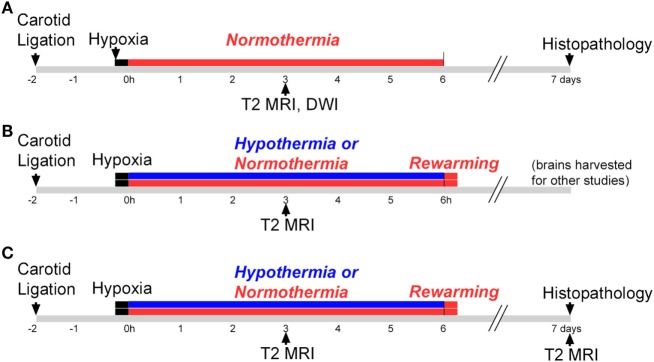
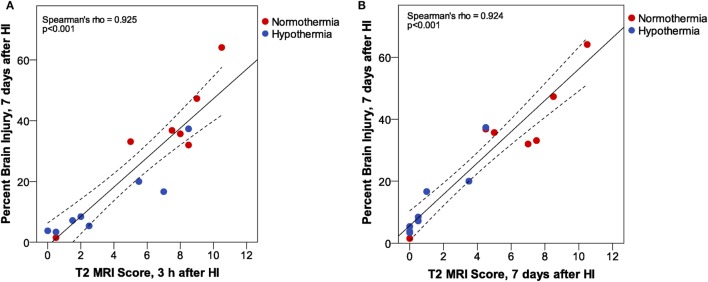
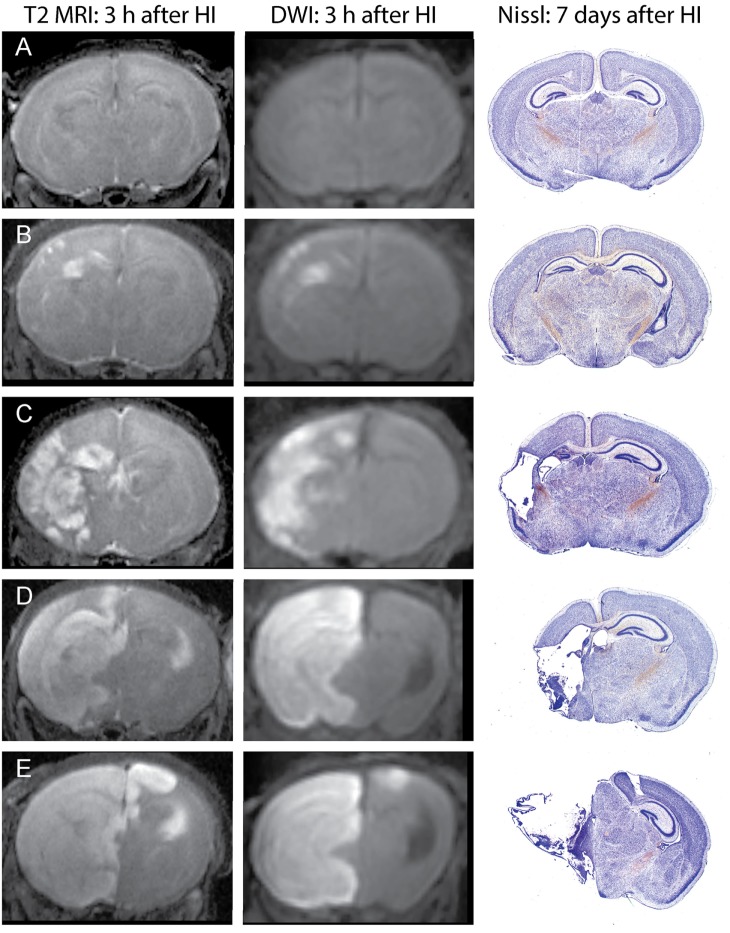
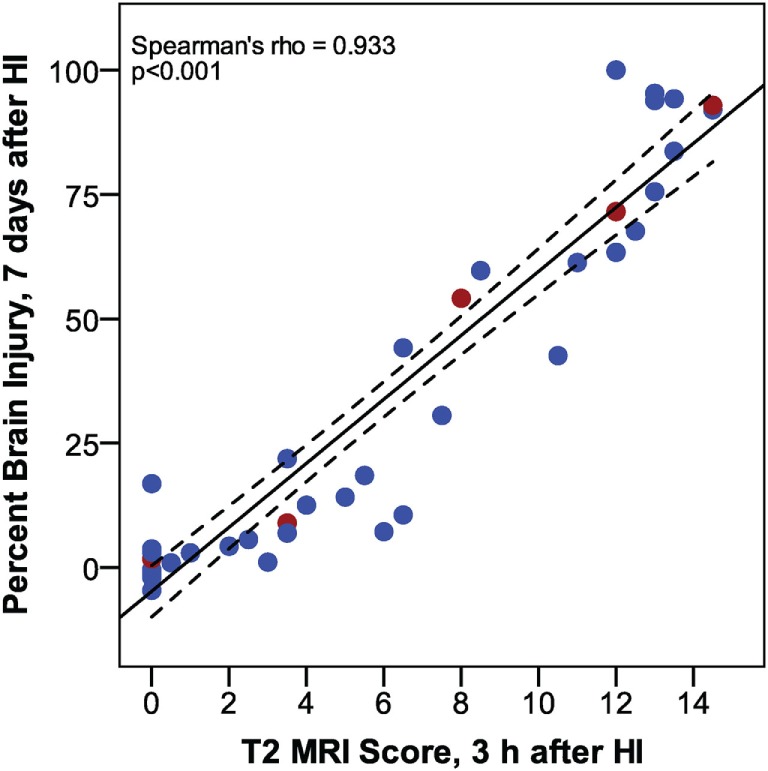
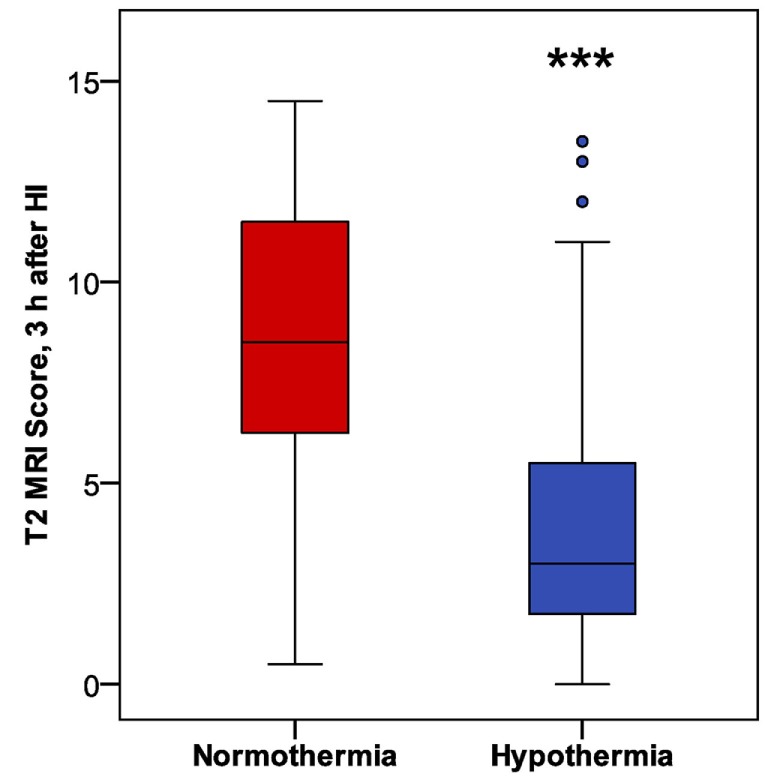
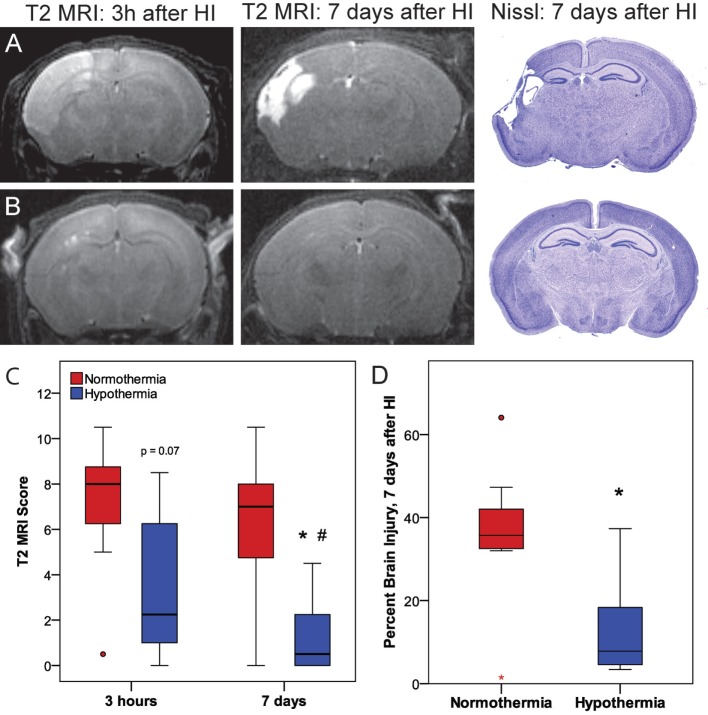
Perinatal hypoxic-ischemic encephalopathy (HIE) can lead to neurodevelopmental disorders, including cerebral palsy. Standard care for neonatal HIE includes therapeutic hypothermia, which provides partial neuroprotection; magnetic resonance imaging (MRI) is often used to assess injury and predict outcome after HIE. Immature rodent models of HIE are used to evaluate mechanisms of injury and to examine the efficacy and mechanisms of neuroprotective interventions such as hypothermia. In this study, we first confirmed that, in the CD1 mouse model of perinatal HIE used for our research, MRI obtained 3 h after hypoxic ischemia (HI) could reliably assess initial brain injury and predict histopathological outcome. Mice were subjected to HI (unilateral carotid ligation followed by exposure to hypoxia) on postnatal day 7 and were imaged with T2-weighted MRI and diffusion-weighted MRI (DWI), 3 h after HI. Clearly defined regions of increased signal were comparable in T2 MRI and DWI, and we found a strong correlation between T2 MRI injury scores 3 h after HI and histopathological brain injury 7 days after HI, validating this method for evaluating initial injury in this model of HIE. The more efficient, higher resolution T2 MRI was used to score initial brain injury in subsequent studies. In mice treated with hypothermia, we found a significant reduction in T2 MRI injury scores 3 h after HI, compared to normothermic littermates. Early hypothermic neuroprotection was maintained 7 days after HI, in both T2 MRI injury scores and histopathology. In the normothermic group, T2 MRI injury scores 3 h after HI were comparable to those obtained 7 days after HI. However, in the hypothermic group, brain injury was significantly less 7 days after HI than at 3 h. Thus, early neuroprotective effects of hypothermia were enhanced by 7 days, which may reflect the additional 3 h of hypothermia after imaging or effects on later mechanisms of injury, such as delayed cell death and inflammation. Our results demonstrate that hypothermia has early neuroprotective effects in this model. These findings suggest that hypothermia has an impact on early mechanisms of excitotoxic injury and support initiation of hypothermic intervention as soon as possible after diagnosis of HIE.
围产期缺氧缺血性脑病(HIE)可导致神经发育障碍,包括脑瘫。新生儿HIE的标准治疗包括治疗性低温,其可提供部分神经保护作用;磁共振成像(MRI)常用于评估HIE后的损伤情况并预测预后。未成熟的啮齿动物HIE模型用于评估损伤机制,并研究低温等神经保护干预措施的疗效和机制。在本研究中,我们首先证实,在我们用于研究的围产期HIE的CD1小鼠模型中,缺氧缺血(HI)后3小时获得的MRI能够可靠地评估初始脑损伤并预测组织病理学结果。在出生后第7天对小鼠进行HI(单侧颈动脉结扎后暴露于缺氧环境),并在HI后3小时用T2加权MRI和扩散加权MRI(DWI)进行成像。T2 MRI和DWI中信号增强的明确区域具有可比性,并且我们发现HI后3小时的T2 MRI损伤评分与HI后7天的组织病理学脑损伤之间存在强相关性,验证了该方法在该HIE模型中评估初始损伤的有效性。在随后的研究中,使用效率更高、分辨率更高的T2 MRI对初始脑损伤进行评分。在接受低温治疗的小鼠中,与体温正常的同窝小鼠相比,我们发现HI后3小时T2 MRI损伤评分显著降低。HI后7天,无论是T2 MRI损伤评分还是组织病理学检查,早期低温神经保护作用均得以维持。在体温正常组中,HI后3小时的T2 MRI损伤评分与HI后7天获得的评分相当。然而,在低温组中,HI后7天的脑损伤明显少于3小时时。因此,低温的早期神经保护作用在7天时增强,这可能反映了成像后额外3小时的低温作用或对后期损伤机制的影响,如延迟性细胞死亡和炎症。我们的结果表明,低温在该模型中具有早期神经保护作用。这些发现提示,低温对兴奋性毒性损伤的早期机制有影响,并支持在诊断HIE后尽快启动低温干预。