Department of Surgery, Dokkyo Medical University, Koshigaya Hospital, 2-1-50, Minami Koshigaya, Koshigaya, Saitama, 343-8555, Japan.
Department of Pathology, Dokkyo Medical University, Koshigaya Hospital, 2-1-50, Minami Koshigaya, Koshigaya, Saitama, 343-8555, Japan.
World J Surg Oncol. 2018 Jun 5;16(1):105. doi: 10.1186/s12957-018-1403-9.
Neoadjuvant chemoradiotherapy (NACRT) has now become the standard treatment for locally advanced rectal cancer (LARC). NACRT has decreased local relapse (LR) rate in patients with LARC; however, distant relapse has recently attracted much attention. This study aimed to assess the feasibility and efficiency of neoadjuvant chemotherapy (NAC) for LARC.
Data on patients with cT3/4 and N+ rectal cancer who were treated in our institution from April 2010 to February 2016 were reviewed retrospectively. Twenty-seven patients who received 2-9 cycles of oxaliplatin-based NAC and 28 patients who received NACRT (45 Gy delivered in 25 fractions and 5-fluorouracil-based oral chemotherapy) were analyzed. The primary and secondary endpoints of the present study were the 3-year relapse-free survival (RFS) and the local and distant relapse rates, respectively.
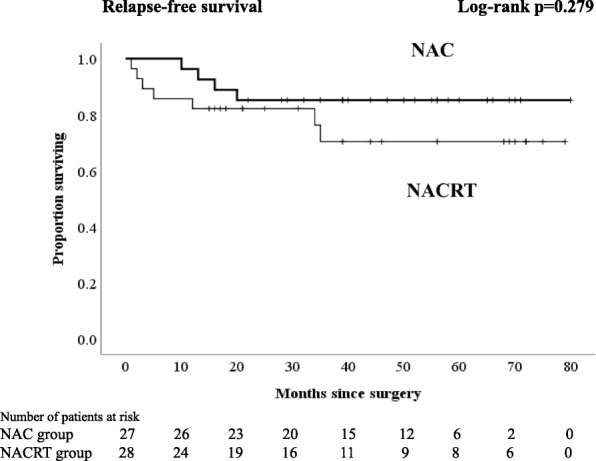
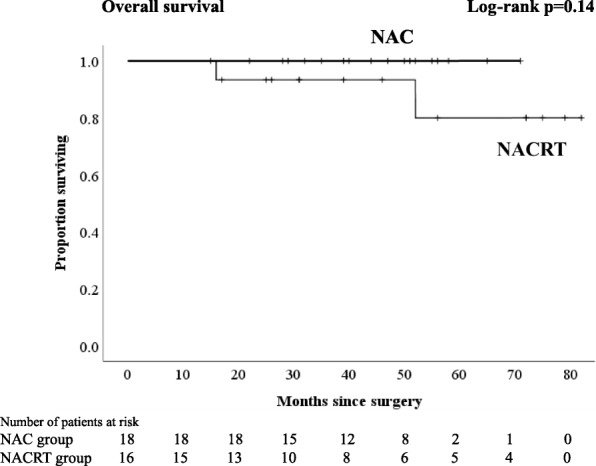
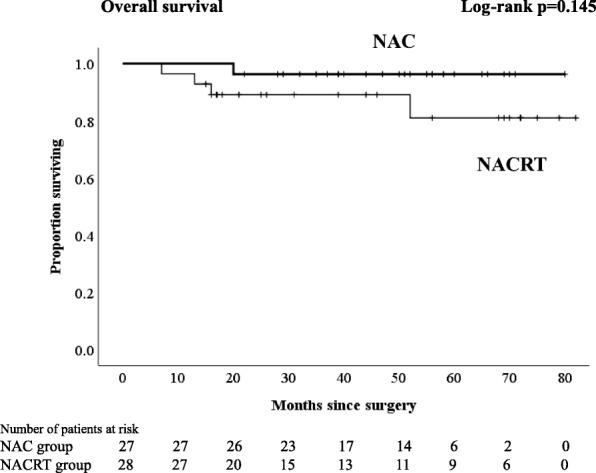
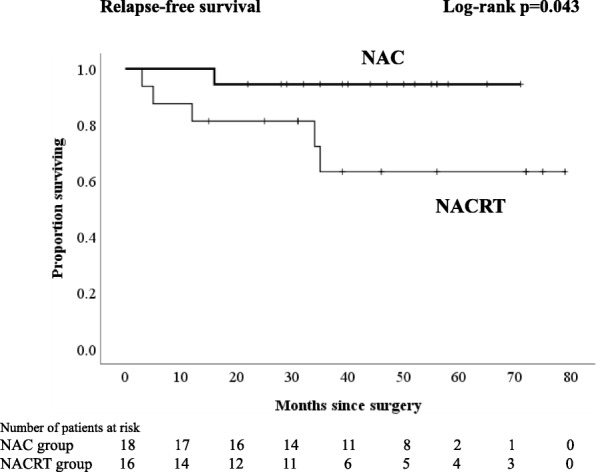
Regardless of the kind of neoadjuvant therapy, no patient experienced any grade 3-4 therapy-related adverse events. The frequent toxic events were grade 1 diarrhea in patients with NACRT and neutropenia in patients with NAC. A significantly higher proportion of patients with NAC underwent laparoscopic surgery and anterior resection (p = 0.037 and p = 0.003, respectively). The percentages of patients with lymph node yield less than 12 in the NAC group, and those in the NACRT group were 26 and 68%, respectively (p = 0.002). Comparing the NAC with the NACRT groups, the local relapse and distant relapse rates were 7.4 and 7.1% and 7.4 and 18%, respectively. There were no significant differences in 3-year RFS and 4-year overall survival (OS) between NAC and NACRT (3-year RFS 85.2 vs. 70.4%, p = 0.279; 4-year OS 96.3 vs. 89.1%, p = 0.145, respectively). With an analysis excluding patients who received postoperative adjuvant chemotherapy, no patients who received NAC had a distant relapse, and there was a significant difference in 3-year RFS compared with the NACRT groups (94.4 vs. 63.2%, p = 0.043).
These outcomes suggest that the therapeutic effect of oxaliplatin-based NAC is at least equal to that of NACRT and that NAC is a feasible and promising option for LARC.
新辅助放化疗(NACRT)现已成为局部晚期直肠癌(LARC)的标准治疗方法。NACRT 降低了局部复发(LR)率,但远处复发率最近引起了广泛关注。本研究旨在评估新辅助化疗(NAC)治疗 LARC 的可行性和疗效。
回顾性分析 2010 年 4 月至 2016 年 2 月在我院接受治疗的 cT3/4 和 N+直肠癌患者的数据。分析了接受 2-9 个周期奥沙利铂为基础的 NAC 治疗的 27 例患者和接受 NACRT(45Gy 分 25 次给予,同时给予氟尿嘧啶类口服化疗)治疗的 28 例患者。本研究的主要和次要终点分别为 3 年无复发生存率(RFS)和局部及远处复发率。
无论采用何种新辅助治疗,均无患者出现任何 3-4 级治疗相关不良事件。NACRT 组患者常出现 1 级腹泻,NAC 组患者常出现中性粒细胞减少。NAC 组中接受腹腔镜手术和前切除术的患者比例明显更高(p=0.037 和 p=0.003)。NAC 组淋巴结检出数<12 的患者比例为 26%,NACRT 组为 68%(p=0.002)。与 NACRT 组相比,NAC 组的局部复发率和远处复发率分别为 7.4%和 7.1%,18%和 18%。NAC 组和 NACRT 组的 3 年 RFS 和 4 年总生存率(OS)无显著差异(3 年 RFS:85.2% vs. 70.4%,p=0.279;4 年 OS:96.3% vs. 89.1%,p=0.145)。在排除接受术后辅助化疗的患者后,接受 NAC 的患者无一例出现远处复发,且与 NACRT 组相比,3 年 RFS 有显著差异(94.4% vs. 63.2%,p=0.043)。
这些结果表明,奥沙利铂为基础的 NAC 的治疗效果至少与 NACRT 相当,NAC 是 LARC 的一种可行且有前途的选择。