Joo Hyung Joon, Jeong Han Saem, Kook Hyungdon, Lee Seung Hun, Park Jae Hyoung, Hong Soon Jun, Yu Cheol Woong, Lim Do-Sum
Department of Cardiology, Cardiovascular Center, Korea University Anam Hospital, 126-1, 5ka, Anam-dong, Sungbuk-ku, Seoul, 136-705, Republic of Korea.
BMC Cardiovasc Disord. 2018 Jun 11;18(1):114. doi: 10.1186/s12872-018-0840-2.
There have been limited data on the impact of hyperuricemia on long-term clinical outcomes after percutaneous coronary intervention (PCI) for in-stent restenosis (ISR).
From January 2009 to July 2015, 317 patients who underwent repeat PCI for ISR were divided into two groups: patients with normal serum uric acid (UA) levels (normal UA group) and patients with higher serum UA levels (higher UA group). The higher UA group included patients with serum UA levels > 6.8 mg/dL or patients who were taking anti-hyperuricemic medication.
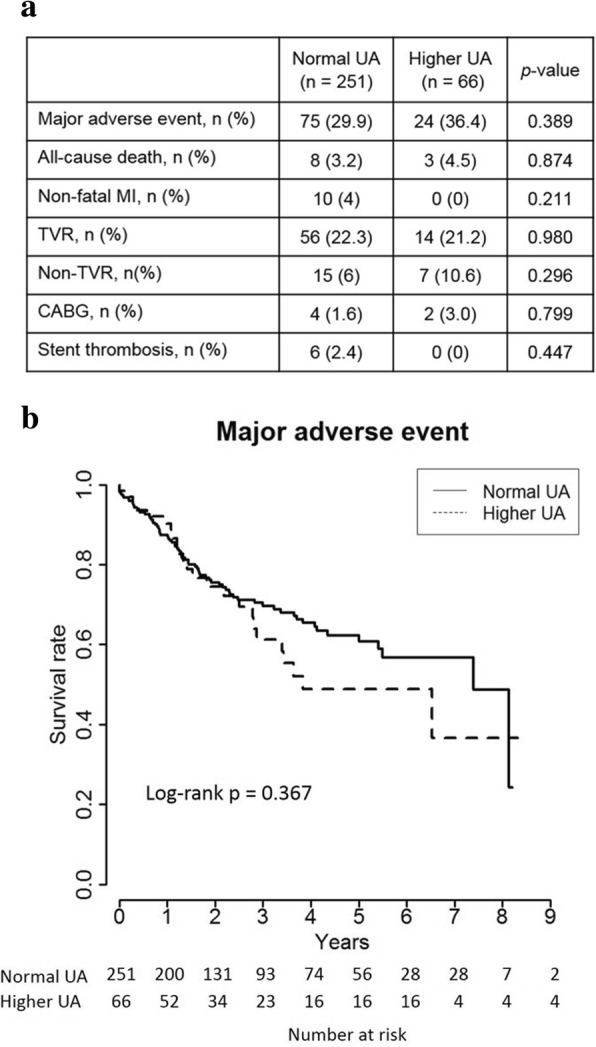
During a median follow-up period of 1088 days, the cumulative incidence rates of major adverse event (MAE), including a composite of all-cause death, non-fatal myocardial infarction, and any revascularization, were similar between the two groups (higher UA 36.4% vs. normal UA 29.9%, p = 0.389, log-rank p = 0.367). Follow-up angiographic data showed similar outcomes of late lumen loss (0.8 ± 0.9 mm vs. 0.8 ± 1.1 mm, p = 0.895) and binary restenosis rate (28.1% vs. 34.7%, p = 0.622). Multivariate Cox regression analysis indicated higher levels of low-density lipoprotein cholesterol (hazard ratio [HR] 1.011, 95% confidence interval [CI] 1.003-1.019, p = 0.006) and lower left ventricular ejection fraction (HR 0.972, 95% CI 0.948-0.996, p = 0.022), but not UA levels, to be the independent risk predictors of MAE.
Hyperuricemia is not associated with poor clinical outcomes after repeat PCI for ISR lesions.
关于高尿酸血症对经皮冠状动脉介入治疗(PCI)后支架内再狭窄(ISR)长期临床结局的影响,相关数据有限。
2009年1月至2015年7月,317例因ISR接受再次PCI的患者被分为两组:血清尿酸(UA)水平正常的患者(正常UA组)和血清UA水平较高的患者(较高UA组)。较高UA组包括血清UA水平>6.8mg/dL的患者或正在服用抗高尿酸血症药物的患者。
在中位随访期1088天内,两组主要不良事件(MAE)的累积发生率相似,MAE包括全因死亡、非致命性心肌梗死和任何血管重建的复合事件(较高UA组为36.4%,正常UA组为29.9%,p=0.389,对数秩检验p=0.367)。随访血管造影数据显示,两组晚期管腔丢失(0.8±0.9mm对0.8±1.1mm,p=0.895)和二元再狭窄率(28.1%对34.7%,p=0.622)的结果相似。多变量Cox回归分析表明,低密度脂蛋白胆固醇水平较高(风险比[HR]1.011,95%置信区间[CI]1.003-1.019,p=0.006)和左心室射血分数较低(HR0.972,95%CI0.948-0.996,p=0.022)是MAE的独立风险预测因素,而非UA水平。
高尿酸血症与ISR病变再次PCI后的不良临床结局无关。