Istanbul Kemerburgaz University, Medical Faculty, Department of Otorhinolaryngology, Tarsus, Turkey.
Medical Park Tarsus Hospital, Radiology, Tarsus, Turkey.
Braz J Otorhinolaryngol. 2019 Sep-Oct;85(5):565-570. doi: 10.1016/j.bjorl.2018.04.010. Epub 2018 May 18.
The most common cause of septoplasty failure is inferior turbinate hypertrophy that is not treated properly. Several techniques have been described to date: total or partial turbinectomy, submucosal resection (surgical or with a microdebrider), with turbinate outfracture being some of those.
In this study, we compared the pre- and postoperative lower turbinate volumes using computed tomography in patients who had undergone septoplasty and compensatory lower turbinate turbinoplasty with those treated with outfracture and bipolar cauterization.
This retrospective study enrolled 66 patients (37 men, 29 women) who were admitted to our otorhinolaryngology clinic between 2010 and 2017 because of nasal obstruction and who were operated on for nasal septum deviation. The patients who underwent turbinoplasty due to compensatory lower turbinate hypertrophy were the turbinoplasty group; Outfracture and bipolar cauterization were separated as the out fracture group. Compensatory lower turbinate volumes of all patients participating in the study (mean age 34.0±12.4 years, range 17-61 years) were assessed by preoperative and postoperative 2 month coronal and axial plane paranasal computed tomography.
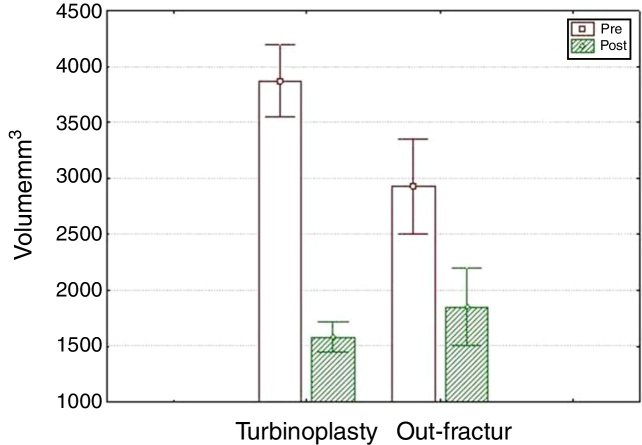
The transverse and longitudinal dimensions of the postoperative turbinoplasty group were significantly lower than those of the out-fracture group (p=0.004). In both groups the lower turbinate volumes were significantly decreased (p=0.002, p<0.001 in order). The postoperative volume of the turbinate on the deviated side of the patients was significantly increased: tubinoplasty group (p=0.033).
Both turbinoplasty and outfracture are effective volume-reduction techniques. However, the turbinoplasty method results in more reduction of the lower turbinate volume than outfracture and bipolar cauterization.
鼻中隔成形术失败的最常见原因是下鼻甲肥大未得到适当治疗。迄今为止,已经描述了几种技术:鼻甲全部或部分切除术、粘膜下切除术(手术或使用微型磨除器),鼻甲外突术就是其中之一。
在这项研究中,我们比较了鼻中隔成形术和下鼻甲代偿性鼻甲成形术患者与下鼻甲外突术和双极电凝术患者的下鼻甲体积的术前和术后 CT 测量值。
这项回顾性研究纳入了 2010 年至 2017 年间因鼻塞而在我们耳鼻喉科诊所就诊并因鼻中隔偏曲而接受手术的 66 例患者(37 名男性,29 名女性)。因下鼻甲代偿性肥大而行鼻甲成形术的患者为鼻甲成形术组;下鼻甲外突术和双极电凝术为外突组。所有参与研究的患者(平均年龄 34.0±12.4 岁,范围 17-61 岁)的下鼻甲体积均通过术前和术后 2 个月的冠状位和轴位鼻窦 CT 进行评估。
鼻甲成形术组的术后鼻甲横径和纵径明显小于外突组(p=0.004)。两组患者的下鼻甲体积均明显减小(p=0.002,p<0.001)。患者偏曲侧鼻甲的术后体积明显增大:鼻甲成形术组(p=0.033)。
鼻甲成形术和下鼻甲外突术都是有效的鼻甲体积缩小技术。然而,鼻甲成形术比下鼻甲外突术和双极电凝术更能减少下鼻甲的体积。